- Indications for END:
- Depth of Invasion (DOI) Thresholds:
- DOI is the single most important predictor:
- Guiding the decision to perform END in cN0 oral cavity SCC
- The NCCN Guidelines stratify the decision as follows [1]:
- DOI 3 mm:
- END should be strongly considered if RT is not already planned (supported by level 1 evidence from the D’Cruz / Tata Memorial trial)
- The landmark D’Cruz et al. (2015) randomized trial of 500 patients with cT1 to T2 cN0 oral cavity SCC:
- Demonstrated that upfront END significantly improved 3-year overall survival (80.0% vs. 67.5%) and disease-specific survival (69.5% vs. 45.9%) compared to therapeutic neck dissection [2]
- Post hoc analysis showed no benefit for tumors with DOI ≤ 3 mm, while 28% of cN0 necks with DOI >3 mm harbored occult metastases [3]
- A 2025 meta-analysis of 17 studies (2,263 patients):
- Confirmed END reduces regional recurrence (RR 0.47) and improves OS (RR 0.75) and DSS (RR 1.32) [4]
- DOI 3 mm:
- A validation study of 300 patients:
- Confirmed that DOI ≥ 4 mm is the optimal ROC-derived threshold (95.1% sensitivity, 52.9% specificity) for predicting occult nodal metastasis:
- With regional recurrence-free survival significantly higher in the END group for DOI ≥ 4 mm (p = 0.002) [5]
- Confirmed that DOI ≥ 4 mm is the optimal ROC-derived threshold (95.1% sensitivity, 52.9% specificity) for predicting occult nodal metastasis:
- A recent systematic review found:
- Diagnostic thresholds converging around 4 mm for mixed oral cavity sites and 3 mm for high-risk subsites (floor of the mouth) [6]
- DOI is the single most important predictor:
- Depth of Invasion (DOI) Thresholds:
- The ASCO Clinical Practice Guideline (2019) recommends [2]:
- cT2 to cT4, cN0:
- Ipsilateral END should be performed (strong recommendation, high-quality evidence)
- cT1, cN0:
- Ipsilateral END should be performed:
- Alternatively, close surveillance with specialized ultrasound may be offered for selected highly reliable patients
- Ipsilateral END should be performed:
- cT2 to cT4, cN0:
- Tumor Size Considerations:
- Under AJCC 8th edition staging, both surface size and DOI determine T classification [1]:
- T1:
- ≤ 2 cm with DOI ≤ 5 mm
- T2:
- ≤ 2 cm with DOI > 5 mm
- > 2 cm and ≤ 4 cm with DOI ≤ 10 mm
- T3 to T4:
- T3:
- > 4 cm
- DOI > 10 mm
- Locally advanced tumors carry ~40% to 50% risk of occult nodal metastases, making END essentially mandatory [2]
- T3:
- T1:
- DOI cutoffs are more predictive of overall survival than T category based on tumor surface size alone [3]:
- For T1 tumors, those with DOI ≤ 2 mm rarely demonstrate occult neck disease:
- While DOI ≥ 2 mm confers at least a 20% risk of pN+ disease [3]
- For T1 tumors, those with DOI ≤ 2 mm rarely demonstrate occult neck disease:
- Under AJCC 8th edition staging, both surface size and DOI determine T classification [1]:
- Subsite-Specific Considerations:
- Oral Tongue:
- The most extensively studied subsite
- DOI ≥ 3 mm to 4 mm:
- Is the standard threshold for END [3]
- Higher propensity for skip metastases:
- To level III (17.5% of specimens) compared to other subsites
- Anterior tongue tumors at / near midline:
- Warrant consideration for bilateral neck dissection [1]
- Floor of Mouth (FOM):
- FOM tumors cross the critical 20% threshold for nodal metastasis at a lower DOI (≥ 2 mm) compared to oral tongue (≥ 4 mm):
- Based on a study of 343 patients:
- 41.7% nodal metastasis rate for FOM tumors 2.1 mm to 4 mm thick vs. 11.2% for tongue tumors of similar thickness [7]
- Based on a study of 343 patients:
- FOM primaries have a predisposition for contralateral metastases even at earlier T stages:
- With a 50% higher risk of contralateral metastasis and 2.6-times higher risk when FOM invasion / extension is present [3][2]
- However, a more recent study of 825 patients:
- Found no significant difference in the incidence of or correlation between DOI and nodal metastases when FOM was compared to other subsites [8]
- SLN biopsy accuracy:
- Is lower for FOM than for tongue primaries [1]
- FOM tumors cross the critical 20% threshold for nodal metastasis at a lower DOI (≥ 2 mm) compared to oral tongue (≥ 4 mm):
- Buccal Mucosa:
- Behaves more aggressively:
- With occult metastasis rates as high as 32% and up to 43% presenting with clinical / radiographic nodal disease [3]
- END is recommended for all buccal cases:
- Irrespective of DOI given higher rates of nodal metastases even in early T-category disease [3]
- A multicenter study of 101 patients confirmed END improved survival in pT2, cN0 buccal SCC:
- 123 months vs. 26 months, p = 0.009) [9]
- END demonstrated improved:
- Locoregional recurrence-free rates (61% vs. 38%, p = 0.042)
- 5-year DFS (75% vs. 63%, p = 0.019) [10]
- Behaves more aggressively:
- Other Subsites (Alveolar Ridge, Retromolar Trigone, Hard Palate):
- Generally follow the same DOI-based principles
- Hard palate and upper gingiva:
- May not lend themselves well to SLN biopsy [1]
- Oral Tongue:
- Levels of Dissection: I to III vs. I to IV:
- This is the NCCN treatment algorithm for cT1 to cT2, N0 oral cavity SCC:
- For the cN0 neck:
- The standard END is a supraomohyoid neck dissection (SOHND) encompassing levels I to III
- Both the NCCN and ASCO guidelines recommend at minimum:
- Levels Ia, Ib, II, and III, with an adequate yield of ≥ 18 lymph nodes [1][2]
- Two randomized trials comparing SOHND (levels I to III) versus modified radical neck dissection (levels I to V):
- Showed the adequacy of SOHND, with more extensive dissection increasing morbidity (particularly shoulder dysfunction) without survival or recurrence benefit:
- Only 3.7% of occult metastases were detected in levels IV and V [2]
- Showed the adequacy of SOHND, with more extensive dissection increasing morbidity (particularly shoulder dysfunction) without survival or recurrence benefit:
- The American Head and Neck Society review consolidates the recommendation:
- Level I to III dissection in the cN0 setting, with consideration of level IV inclusion in higher-risk tumors [3]
- For the cN0 neck:
- This is the NCCN treatment algorithm for cT1 to cT2, N0 oral cavity SCC:
- Skip Metastasis to Level IV:
- The Key Data:
- The Warshavsky et al. (2019) systematic review and meta-analysis in JAMA Otolaryngology (13 studies, 1,359 patients) provides the most comprehensive data [11]:
- Overall rate of level IV involvement in cN0 patients:
- 2.53% (95% CI, 1.64%–3.55%)
- True skip metastasis rate:
- Level IV positive without levels I to III involvement): 0.50% (95% CI, 0.09%–1.11%)
- Overall rate of level IV involvement in cN0 patients:
- The Warshavsky et al. (2019) systematic review and meta-analysis in JAMA Otolaryngology (13 studies, 1,359 patients) provides the most comprehensive data [11]:
- Subgroup by T stage:
- Level IV involvement was 0% for stages I to II and 0% for stages III to IV in the skip metastasis analysis
- Oral tongue subsite:
- Level IV involvement was notably higher at 3.60% (95% CI, 2.09%–5.42%):
- The only subsite with significant findings
- A large audit of 1,004 cases:
- Confirmed skip metastases to level IV were 2.2% for tongue and 1.2% for gingivobuccal primaries [12]
- A 2024 study of 544 early-stage oral tongue SCC patients:
- Found only 1.3% had nodal involvement of level IV or V, concluding that END of levels I to III is sufficient [13]
- A recent 2026 study directly comparing outcomes of END levels I to III vs. I to IV in 120 oral tongue SCC patients found [14]:
- Only 1 of 33 patients (3%) undergoing level I to IV dissection had level IV metastasis
- No significant difference in regional recurrence (21.8% vs. 18.2%, p = 0.66), level IV recurrence (3.5% vs. 3%, p = 0.91), or 5-year OS (69.3% vs. 61.1%, p = 0.7)
- However, one study of 111 T1 / T2 N0 oral tongue SCC patients:
- Found a 6.3% occult metastasis rate to level IV:
- Arguing that extended SOHND covers this risk [15]
- Found a 6.3% occult metastasis rate to level IV:
- Additionally, when levels I to III are already pN+:
- The risk of level IV to V metastases rises to 9.8%:
- Particularly with > 1 positive node or pN classification > pN2b [16]
- The risk of level IV to V metastases rises to 9.8%:
- Level IV involvement was notably higher at 3.60% (95% CI, 2.09%–5.42%):
- The Key Data:
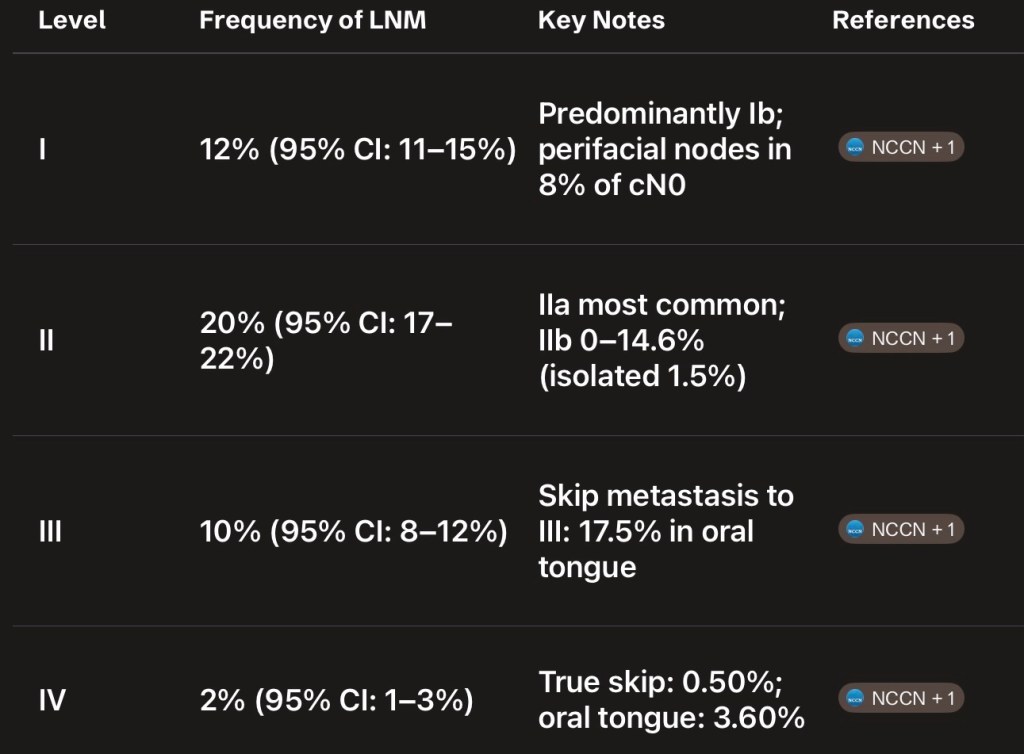
- Summary of Frequency of Nodal Metastasis by Level:
- A meta-analysis of 17 studies found the following frequencies of lymph node metastasis across all OSCC [17] – Figure
- Clinical Synthesis:
- For the cN0 neck, levels I to III dissection is the standard of care across all oral cavity subsites
- The evidence does not support routine inclusion of level IV given the extremely low rate of true skip metastasis (0.50% overall)
- For oral tongue SCC specifically:
- The slightly higher rate of level IV involvement (3.60%) has prompted some authors to advocate for level IV inclusion:
- But direct comparative studies show no survival or recurrence benefit from extending to level IV [14]
- The slightly higher rate of level IV involvement (3.60%) has prompted some authors to advocate for level IV inclusion:
- Level IV should be considered in higher-risk scenarios:
- pN+ disease in levels I to III (especially multistation), greater DOI, or adverse pathologic features
- For the cN+ neck:
- Therapeutic dissection should include levels I to IV:
- With level V considered in multistation disease [2]
- Therapeutic dissection should include levels I to IV:
- References:
- 1. Head and Neck Cancers. National Comprehensive Cancer Network. Updated 2025-12-08.
- 2. Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. Koyfman SA, Ismaila N, Crook D, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(20):1753-1774. doi:10.1200/JCO.18.01921.
- 3. Oral Cavity Cancer Surgical and Nodal Management: A Review From the American Head and Neck Society. Eskander A, Dziegielewski PT, Patel MR, et al. JAMA Otolaryngology– Head & Neck Surgery. 2024;150(2):172-178. doi:10.1001/jamaoto.2023.4049.
- 4. Impact of Elective Cervical Dissection on the Prognosis of Patients With Oral Squamous Cell Carcinoma cT1/T2N0: A Systematic Review and Meta-Analysis. Binda NC, Lavareze L, de Souza Vieira G, et al. Critical Reviews in Oncology/Hematology. 2025;:104982. doi:10.1016/j.critrevonc.2025.104982.
- 5. Depth of Invasion in Early Stage Oral Cavity Squamous Cell Carcinoma: The Optimal Cut-Off Value for Elective Neck Dissection. van Lanschot CGF, Klazen YP, de Ridder MAJ, et al. Oral Oncology. 2020;111:104940. doi:10.1016/j.oraloncology.2020.104940.
- 6. Elective Neck Dissection Strategies Guided by AJCC-8 Depth-of-Invasion (DOI) in cT1-T2N0 Oral Cavity Cancer-a Systematic Review. Abdul NS, Shivakumar S, Alreshaid L, et al. Cancers. 2026;18(4):697. doi:10.3390/cancers18040697.
- 7. Tumour Thickness as a Predictor of Nodal Metastases in Oral Cancer: Comparison Between Tongue and Floor of Mouth Subsites. Balasubramanian D, Ebrahimi A, Gupta R, et al. Oral Oncology. 2014;50(12):1165-8. doi:10.1016/j.oraloncology.2014.09.012.
- 8. The Relative Propensity for Regional Metastasis in Floor of Mouth Squamous Cell Carcinoma Versus Other Oral Cavity Subsites. Wicks C, Zubair F, Ogunbowale A, McMahon J. The British Journal of Oral & Maxillofacial Surgery. 2022;60(9):1276-1278. doi:10.1016/j.bjoms.2022.07.012.
- 9. Management of the Neck in T1 and T2 Buccal Squamous Cell Carcinoma. Nicholson OA, Van Lanschot CGF, van den Besselaar BN, et al. International Journal of Oral and Maxillofacial Surgery. 2024;53(4):259-267. doi:10.1016/j.ijom.2023.07.004.
- 10. What Is the Role of Elective Neck Dissection in the Management of Patients With Buccal Squamous Cell Carcinoma and Clinically Negative Neck?. Dillon JK, Villing AS, Jones RS, et al. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2019;77(3):641-647. doi:10.1016/j.joms.2018.10.021.
- 11. Assessment of the Rate of Skip Metastasis to Neck Level IV in Patients With Clinically Node-Negative Neck Oral Cavity Squamous Cell Carcinoma: A Systematic Review and Meta-analysis. Warshavsky A, Rosen R, Nard-Carmel N, et al. JAMA Otolaryngology– Head & Neck Surgery. 2019;145(6):542-548. doi:10.1001/jamaoto.2019.0784.
- 12. Nodal Yield and Topography of Nodal Metastases From Oral Cavity Squamous Cell Carcinoma – An Audit of 1004 Cases Undergoing Primary Surgical Resection. Roy P, Mallick I, Arun I, et al. Oral Oncology. 2021;113:105115. doi:10.1016/j.oraloncology.2020.105115.
- 13. Risk Factors and Impact of Occult and Skip Metastasis in Early-Stage Oral Tongue Squamous Cell Carcinoma. Yang X, Xiang W, Sun Y, et al. Clinical Oral Investigations. 2024;28(9):510. doi:10.1007/s00784-024-05897-8.
- 14. The Prognostic Significance of Elective Level 4 Neck Dissection in Oral Tongue Cancer. Yosefof E, Edri N, Ritter A, et al. Journal of Surgical Oncology. 2026;133(4):459-464. doi:10.1002/jso.70191.
- 15. How Adequate Is Supraomohyoid Neck Dissection for Node-Negative Oral Tongue Squamous Cell Carcinoma?. Sharma R, Singh N, Joshi KD, Sr A, Patrikar S. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2025;:S1010-5182(25)00102-7. doi:10.1016/j.jcms.2025.03.006.
- 16. In Vivo Probability of Metastases in Levels IV-V in Oral Squamous Cell Carcinoma With a cN0/pN+ Situation in Levels I-Iii. Haas L, Mischkowski RA, Knape U, Król KM, Sakkas A. In Vivo (Athens, Greece). 2025 Nov-Dec;39(6):3437-3444. doi:10.21873/invivo.14141.
- 17. Frequency of Lymph Node Metastases at Different Neck Levels in Patients With Oral Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Yu YF, Cao LM, Li ZZ, et al. International Journal of Surgery (London, England). 2025;111(1):1285-1300. doi:10.1097/JS9.0000000000001953.