- A novel nomenclature to classify parathyroid adenomas:
- World Journal of Surgery. 2009;33(3):412–416
- Background and Rationale:
- Traditional descriptions of parathyroid adenomas (e.g., “left inferior,” “ectopic”):
- Are inconsistent and often imprecise:
- Particularly in reoperative surgery or when imaging is discordant
- Are inconsistent and often imprecise:
- Problem:
- Variable embryologic descent → unpredictable locations
- Poor communication between surgeons, radiologists, and endocrinologists
- Difficulty standardizing outcomes and reporting
- Goal of Perrier et al:
- Develop a standardized, anatomically reproducible nomenclature based on predictable embryologic migration patterns
- Traditional descriptions of parathyroid adenomas (e.g., “left inferior,” “ectopic”):
- Embryologic Basis (Core Concept)


- During the fifth to sixth week of intrauterine development:
- The embryonic pharynx is marked:
- Externally by:
- Four branchial clefts of ectoderm origin
- Internally by:
- Five branchial pouches of endoderm origin
- Externally by:
- The branchial apparatus is made up by:
- The branchial clefts and branchial pouches:
- Together with the branchial arches of mesoderm origin:
- Found in between them
- Together with the branchial arches of mesoderm origin:
- The branchial clefts and branchial pouches:
- This apparatus undergoes normal involution:
- Leaving behind some derivatives which include the:
- Thyroid gland, parathyroid glands, thymus, ultimobranchial body, Eustachian tube, middle ear, and external auditory canal
- Leaving behind some derivatives which include the:
- The embryonic pharynx is marked:
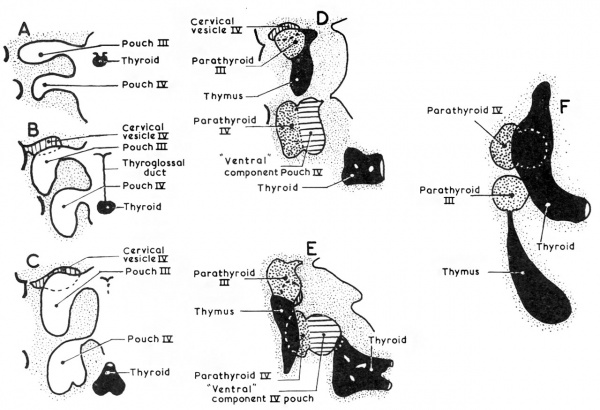
- The parathyroid glands:
- Develop as epithelial thickenings of the dorsal endoderm of the:
- Third and fourth branchial pouches
- The superior parathyroid glands:
- Are derived from the fourth branchial pouch:
- Which also gives rise to the ultimobranchial bodies:
- The ventral aspect of these pouches is believed to fuse with the rudimentary fifth branchial pouches:
- To from the ultimobranchial bodies
- The ventral aspect of these pouches is believed to fuse with the rudimentary fifth branchial pouches:
- Which also gives rise to the ultimobranchial bodies:
- The superior parathyroid glands follow the migration of the ultimobranchial bodies:
- Which descend a relative limited path toward the lateral thyroid region:
- Ultimately giving rise to the parafollicular cells of the thyroid
- The superior parathyroid glands separate from the ultimobranchial bodies:
- As the median and lateral thyroid anlages fuse and incorporate the ultimobranchial bodies:
- This separation event determines the final anatomic position of the superior parathyroid glands relative to the thyroid (Type A gland)
- As the median and lateral thyroid anlages fuse and incorporate the ultimobranchial bodies:
- Which descend a relative limited path toward the lateral thyroid region:
- Are derived from the fourth branchial pouch:
- The inferior parathyroid glands:
- Are derived from the third branchial pouch:
- Along with the thymus (derived from the ventral aspect of the third branchial pouch)
- Are derived from the third branchial pouch:
- Develop as epithelial thickenings of the dorsal endoderm of the:
- The parathyroid glands:
- Remain intimately connected with their respective branchial pouch derivatives
- The normal anatomic location of the superior parathyroid glands:
- Is more constant than the inferior parathyroid glands:
- With 80% of the superior glands being found near the posterior aspect of the thyroid gland:
- At the junction of the upper and middle portion of the thyroid lobes:
- At the level of the cricoid cartilage (each gland with its own capsule of connective tissue):
- Type A gland
- At the level of the cricoid cartilage (each gland with its own capsule of connective tissue):
- At the junction of the upper and middle portion of the thyroid lobes:
- With 80% of the superior glands being found near the posterior aspect of the thyroid gland:
- Roughly one percent (1%) of the superior parathyroid glands:
- May be found in the paraesophageal or retroesophageal space, retrolaryngeal space, high lateral pharyngeal, and carotid shealth locations
- Type B glands:
- Behind the thyroid parenchyma:
- Type B glands are exophytic to the thyroid parenchyma:
- Lie in the tracheoesophageal groove
- Type B glands are exophytic to the thyroid parenchyma:
- Behind the thyroid parenchyma:
- Type C glands:
- Caudal to the thyroid parenchyma, in the tracheoesophageal groove
- A type C gland is more inferior than a type B gland on lateral images and located inferior to the inferior pole of the thyroid (closer to the clavicle).
- Type B glands:
- May be found in the paraesophageal or retroesophageal space, retrolaryngeal space, high lateral pharyngeal, and carotid shealth locations
- Enlarged superior glands:
- May descend in the tracheoesophageal groove and come to lie below the inferior parathyroid glands (Type C gland)
- Truly ectopic superior parathyroid glands:
- Are extremely rare:
- But may be localized to the middle or posterior mediastinum or in the aortopulmonary window
- Are extremely rare:
- Is more constant than the inferior parathyroid glands:
- During intrauterine development:
- The thymus and the inferior parathyroid glands:
- Migrate caudally in the neck
- The most common location for the inferior parathyroid glands:
- Is within 1 cm from a point centered where the inferior thyroid artery and the recurrent laryngeal nerve (RLN) cross
- In roughly 50% of the cases:
- The inferior parathyroid gland is located at the level of the inferior thyroid lobe:
- Anterior of the posterolateral surface:
- Type E:
- Located in the external aspect of the inferior pole of the thyroid
- A type E gland is in a location that is more superficial in an anterior-posterior plane than the recurrent laryngeal nerve
- It is the easiest to resect
- Type E:
- Anterior of the posterolateral surface:
- The inferior parathyroid gland is located at the level of the inferior thyroid lobe:
- Approximately 15% to 50% of the inferior glands:
- Are found in the thyrothymic ligament or the thymus
- The inferior parathyroid gland is typically situated within a pocket of thymic derived fatty tissue:
- But may be closely adherent to the thyroid capsule
- The position of the inferior parathyroid glands:
- However, tends to be more variable due to their longer migratory route:
- Undescended inferior glands may be found near the:
- Skull base, angle of the mandible, or above the superior parathyroid glands:
- Along with an undescended thymus
- Skull base, angle of the mandible, or above the superior parathyroid glands:
- Undescended inferior glands may be found near the:
- However, tends to be more variable due to their longer migratory route:
- The frequency of intrathyroidal glands:
- Is approximately 2%
- The thymus and the inferior parathyroid glands:
- Superior parathyroid glands (4th branchial pouch):
- Short migration
- More constant location
- Posterior to RLN, near cricothyroid joint
- Inferior glands (3rd branchial pouch):
- Long migration with thymus
- Highly variable
- Can be anywhere from angle of mandible → mediastinum
- The classification is built on this predictable vs variable descent pattern
The Perrier Classification System
The authors propose categorizing adenomas based on their relationship to key anatomic landmarks, especially:
- Thyroid gland
- Recurrent laryngeal nerve (RLN)
- Thymus
- Carotid sheath
📍 Four Main Categories
Type A — Orthotopic (Normal Position)


- Located in expected anatomical position
- Adjacent to thyroid gland
- Most common
👉 Clinical relevance:
- Ideal for minimally invasive parathyroidectomy (MIP)
- High concordance with sestamibi + ultrasound
Type B — Ectopic but Cervical



Includes:
- Retroesophageal
- Carotid sheath
- Intrathyroidal
- High cervical (undescended)
👉 Key point: Still in the neck but outside usual location
👉 Surgical implication:
- May require focused but modified approach
- Intrathyroidal → partial thyroid resection
Type C — Thymic / Thyrothymic



- Along thymic descent pathway
- Thyrothymic ligament
- Within cervical thymus or upper mediastinum
👉 Most common ectopic site for inferior glands
👉 Surgical implication:
- Cervical thymectomy often required
- Important in failed initial exploration
Type D — Mediastinal


- Below thoracic inlet
- Aortopulmonary window, pericardium, deep thymus
👉 Rare but critical
👉 Surgical implication:
- May require:
- VATS
- Sternotomy
- Interventional radiology localization
📊 Key Findings from Perrier et al.
- Majority of adenomas are Type A (orthotopic)
- Ectopic locations (Types B to D) account for:
- ~15% to 20% of cases
- Inferior glands → disproportionately represented in ectopic group
👉 The classification correlates strongly with:
- Embryology
- Preoperative imaging success
- Surgical difficulty
🎯 Clinical Impact
1. Improves Communication
- Standard language across:
- Surgeons
- Radiologists
- Endocrinologists
2. Enhances Preoperative Planning
- Predicts:
- Likelihood of MIP vs BNE
- Need for extended exploration
3. Reduces Failed Explorations
- Particularly valuable in:
- Reoperative cases
- Discordant imaging
4. Facilitates Research Standardization
- Enables:
- Comparable outcome reporting
- Better stratification in studies
🧠 Surgical Algorithm Integration
| Imaging Result | Likely Type | Strategy |
|---|---|---|
| Concordant US + Sestamibi | Type A | Focused MIP |
| Discordant imaging | Type B / C | Extended cervical exploration |
| Negative imaging | Type C / D | Consider 4D-CT, PET, BNE |
| Prior failed surgery | Any (often B to D) | Systematic re-exploration |
⚠️ Limitations of the Study
- Retrospective classification
- Single-institution experience (MD Anderson)
- No direct comparison with alternative systems
- Does not incorporate modern imaging (e.g., 4D-CT, PET)
📚 Key References
- Perrier ND et al. World J Surg. 2009;33:412–416
- Akerström G et al. Anatomy and embryology of parathyroid glands. World J Surg. 1984
- Wang C. Parathyroid gland location study (645 cases). Ann Surg. 1976
- Kunstman JW et al. Parathyroid localization techniques. J Surg Oncol. 2013
- Cheung K et al. 4D-CT in parathyroid localization. Radiology. 2012
💡 Take-Home Messages (Chairman-Level)
- This classification is simple, reproducible, and embryology-driven
- Helps predict surgical complexity before incision
- Particularly powerful in:
- Reoperative parathyroid surgery
- Ectopic gland localization
- Should be integrated into:
- Operative reports
- Radiology reporting
- Multidisciplinary discussions

