- Differential Diagnosis of Hypercalcemia:
- Primary hyperparathyroidism:
- Solitary adenoma:
- 85% to 90% of the cases
- Multigland Disease:
- Multigland hyperplasia:
- 3% of the cases
- Doble adenoma:
- 6% to 9% of the cases
- Triple adenoma:
- 0.3% of the cases
- Multigland hyperplasia:
- Solitary adenoma:
- Secondary hyperparathyroidism
- Tertiary hyperparathyroidism
- Familial hypocalciuric hypercalcemia
- Medications:
- Lithium
- Hydrochlorothiazide
- Malignancy:
- Parathyroid carcinoma
- Multiple myeloma
- Tumors producing PTH-related peptide:
- Ovarian cancer
- Lung cancer
- Acute or chronic leukemia
- Granulomatous diseases:
- Sarcoidosis, histioplasmosis, tuberculosis
- Thyrotoxicosis
- Paget disease
- Increased intake:
- Milk-alkali syndrome
- Vitamin A toxicity
- Vitamin D toxicity
- Primary hyperparathyroidism:
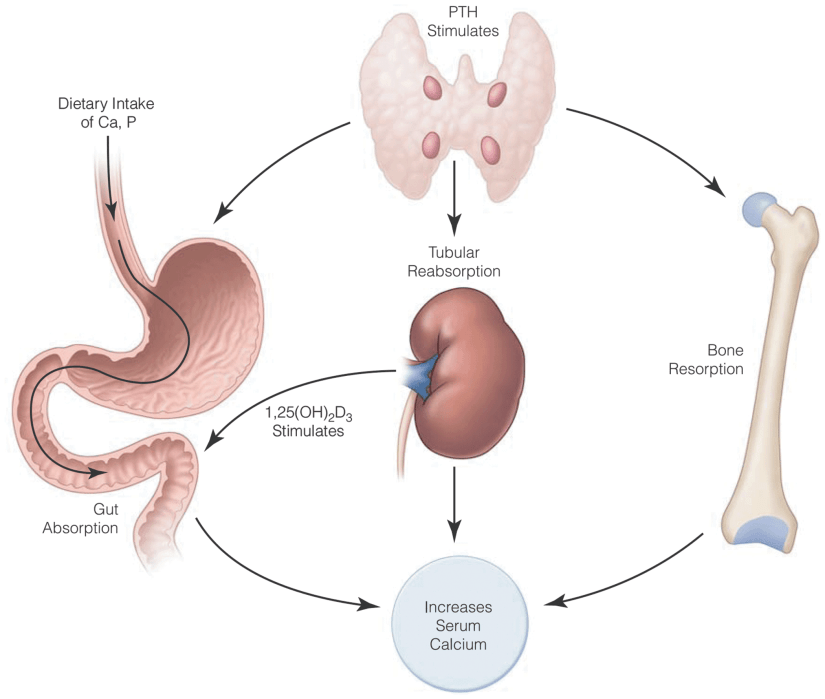
- Primary hyperparathyroidism (PHPT):
- Is caused by an inappropriate, autonomous secretion of parathyroid hormone (PTH) by the parathyroid gland(s):
- Which leads to an elevated serum calcium concentration or wide variations of the serum calcium concentration
- Single gland disease:
- Caused by a single, enlarged, overactive gland, is found in 85% to 90% of cases
- Multiple gland disease occurs in 10% to 15% of the cases:
- Multiple gland disease may consist of:
- Double adenomas (6% to 9% of the cases)
- Four-gland hyperplasia (3% of the cases)
- Three enlarged and one normal appearing gland (0.3% of the cases).
- Because asymmetric hyperplasia is common, it is difficult to distinguish between multiple adenomas and hyperplasia and the term multiple gland disease is preferred
- Multiple gland disease may consist of:
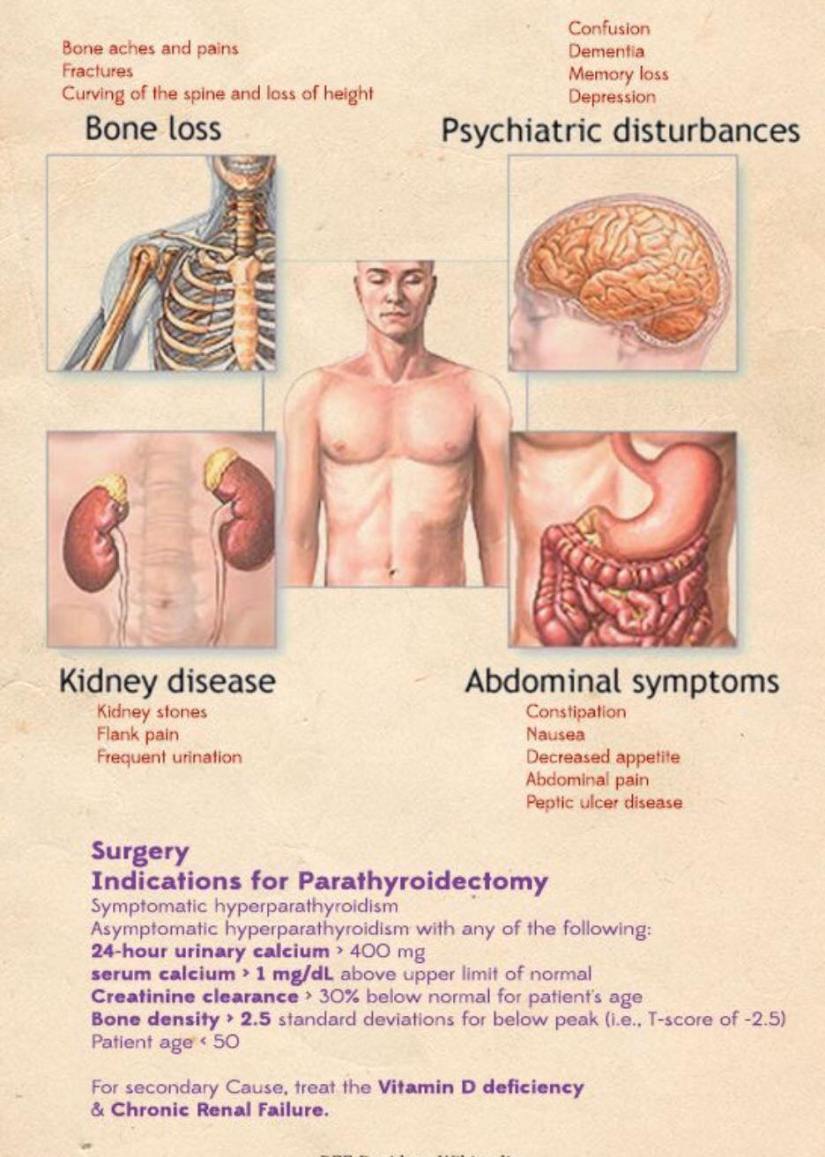
- PHPT in the United States usually presents quite early:
- Often when hypercalcemia is noted during routine laboratory testing
- Signs may include:
- Nephrolithiasis, decreased bone density, and fragility fractures, and subjective symptoms may include fatigue, cognitive changes, depression, constipation and other gastrointestinal complaints, musculoskeletal pain, nocturia, and rarely pruritus:
- Many patients may appear asymptomatic:
- A detailed history often uncovers symptoms:
- 95% of the cases have symptoms when appropriate history is taken:
- The recently revised guidelines for asymptomatic PHPT include a more extensive evaluation of the skeletal and renal systems
- 95% of the cases have symptoms when appropriate history is taken:
- A detailed history often uncovers symptoms:
- Many patients may appear asymptomatic:
- Nephrolithiasis, decreased bone density, and fragility fractures, and subjective symptoms may include fatigue, cognitive changes, depression, constipation and other gastrointestinal complaints, musculoskeletal pain, nocturia, and rarely pruritus:
- A family history of endocrine disorders should be investigated:
- As hyperparathyroidism alone can be familial or can present as a component of multiple endocrine neoplasia (MEN) types 1 and 2A
- Is caused by an inappropriate, autonomous secretion of parathyroid hormone (PTH) by the parathyroid gland(s):






Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello / cirugia endocrina miembro del equipo de Mount Sinai Medical Center experto en el manejo del hiperparatiroidismo primario.
Entrenamiento:
-
Cirugia general y gastrointestinal:
• Michigan State University:
• 2004 al 2010
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Maestria en ciencias (Clinical research for healthprofessionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#CirugiadeTumoresdeCabezayCuello
#CirugiaEndocrina
#CirugiaOncologica
#HeadandNeckSurgery
#EndocrineSurgery
#SurgicalOncology
#Hiperparatiroidismo
#Hyperparathyroidsim
#MountSInaiMedicalCenter
#MSMC
#Mexico #Miami
