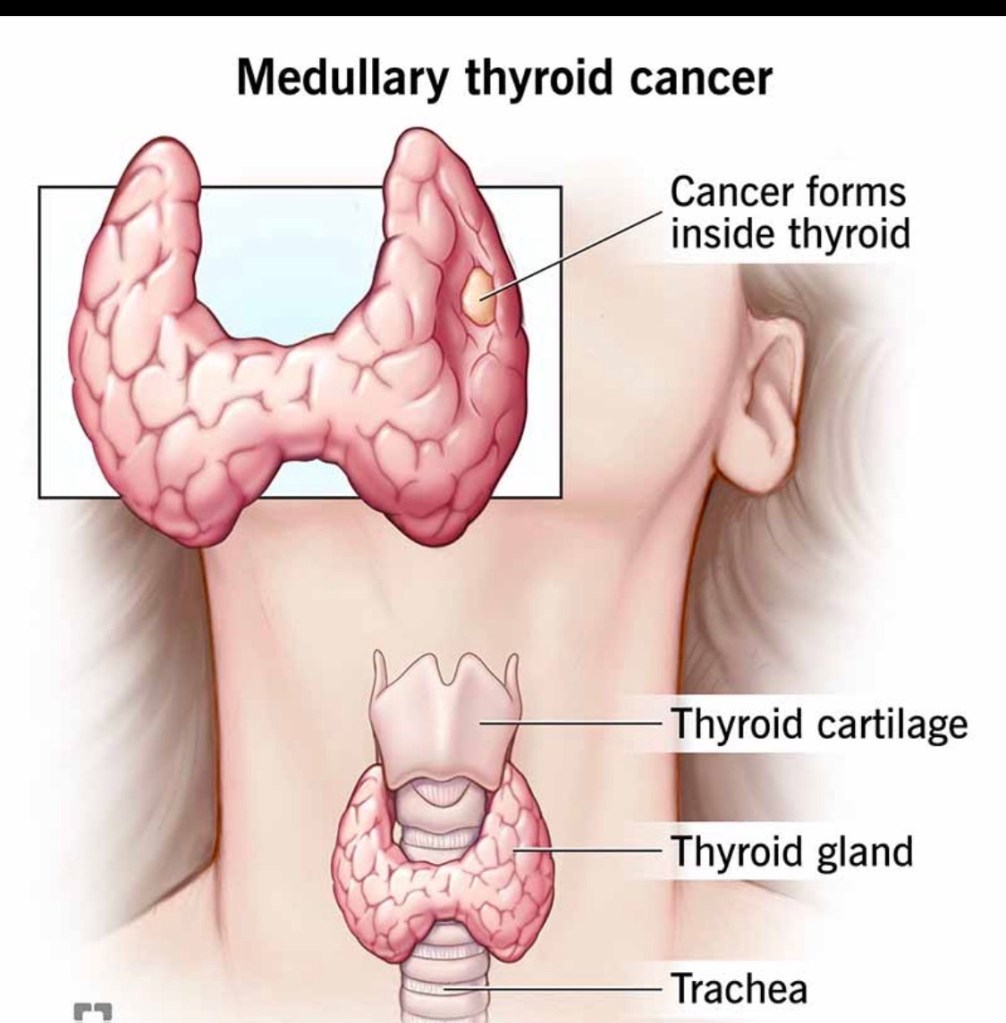
Medullary thyroid cancer (MTC) accounts for ~2–4% of all thyroid cancers and is biologically distinct from papillary and follicular thyroid cancers.
🧠 What makes MTC different?
Arises from parafollicular (C) cells, not follicular cells Produces calcitonin, a key tumor marker Does NOT respond to radioactive iodine Can be sporadic (~75%) or hereditary (~25%)
🧬 The genetic connection
Hereditary MTC is associated with RET mutations Seen in MEN2 syndromes (MEN2A, MEN2B, FMTC) All patients with MTC should undergo genetic testing, regardless of age or family history
🔍 How is MTC diagnosed?
Suspicious thyroid nodule on ultrasound Elevated serum calcitonin (often markedly high) Confirmed by FNA biopsy ± calcitonin washout Imaging to evaluate lymph node involvement
⚖️ How is MTC treated?
The cornerstone of treatment is surgery:
Total thyroidectomy Central neck lymph node dissection Lateral neck dissection when nodes are involved
➡️ Radioactive iodine has no role in MTC.
➡️ Targeted systemic therapies are used in advanced disease.
📈 Prognosis
Highly dependent on stage at diagnosis Early detection → excellent long-term outcomes Lymph node and distant spread worsen prognosis
🦋 Early recognition and expert surgical management are critical.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Medullary thyroid cancer is rare but requires prompt diagnosis, genetic evaluation, and expert surgical care.
📚 References
Wells SA et al. Revised ATA Guidelines for Medullary Thyroid Carcinoma. Thyroid Elisei R et al. Management of Medullary Thyroid Cancer. Lancet NCCN Guidelines: Thyroid Carcinoma
My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
View all posts by Rodrigo Arrangoiz MS, MD, FACS, FSSO