
- Historically, even thin melanomas were excised with very wide margins (3 cm to 5 cm):
- Studies have demonstrated, however, that narrower margins are often associated with the same recurrence rates as wider margins

- For thin melanomas:
- The first randomized study involving surgical margins for melanomas less than 2 mm thick was reported by the WHO Melanoma Group:
- In an update of the study including 612 patients randomly assigned to a 1-cm or 3-cm margin of excision:
- There were no local recurrences among patients with primary melanomas thinner than 1 mm
- In an update of the study including 612 patients randomly assigned to a 1-cm or 3-cm margin of excision:
-
-
- There were four local recurrences among the 100 patients with melanomas 1 to 2 mm thick:
- All four occurred in patients with 1-cm margins
- There was no significant difference in survival between the 1- and 3-cm surgical margin groups
- There were four local recurrences among the 100 patients with melanomas 1 to 2 mm thick:
- These results demonstrate that a 1-cm excision margin is safe for thin (less than 1 mm thick) melanomas
-
- A multi-institutional prospective randomized trial from France:
- Compared 2-cm and 5-cm excisional margins in 362 patients with melanomas less than 2 mm thick:
- There were no differences in local recurrence rate or survival between the two groups
- Compared 2-cm and 5-cm excisional margins in 362 patients with melanomas less than 2 mm thick:
- A randomized trial from Sweden compared 989 melanoma patients with lesions less than 2 mm thick excised with 2-cm and 5-cm margins:
- The results were similar:
- No differences in local recurrence rate or survival between the two groups
- The results were similar:
- The first randomized study involving surgical margins for melanomas less than 2 mm thick was reported by the WHO Melanoma Group:
- For thicker melanomas:
- A randomized clinical trial from the United Kingdom, the United Kingdom Melanoma Study Group (UKMSG) Trial:
- Compared 1-cm and 3-cm excisional margins in 900 patients with melanomas at least 2 mm thick:
- With a median follow-up time of 60 months:
- Compared 1-cm and 3-cm excisional margins in 900 patients with melanomas at least 2 mm thick:
-
-
-
- A 1-cm margin was associated with a significantly increased risk of locoregional recurrence:
- 37% vs. 32% for 3-cm margins
- However, overall survival (OS) was similar in the two groups
- A 1-cm margin was associated with a significantly increased risk of locoregional recurrence:
-
-
- A randomized clinical trial from the United Kingdom, the United Kingdom Melanoma Study Group (UKMSG) Trial:
- For intermediate thickness melanomas:
- A randomized prospective study conducted by the Intergroup Melanoma Committee compared 2-cm and 4-cm radial margins of excision for 1-mm to 4-mm thickness melanomas:
- There was no difference in local recurrence rate between the two groups:
- 46% of patients in the 4-cm group required skin grafts
- There was no difference in local recurrence rate between the two groups:
-
-
- Only 11% of patients in the 2-cm group:
- P < 0.001
- Only 11% of patients in the 2-cm group:
- A trend for improved 10-year disease-specific survival was seen in 4-cm margins (77%) versus 2-cm margins (70%)
-
- A clinical trial directly comparing 1-cm and 2-cm margins for 1-mm to 2-mm melanomas has not been performed:
- Based upon data from the WHO Trial and the Intergroup Melanoma Trial:
- 2-cm margins are recommended when the anatomic location is favorable and primary closure can be achieved
- Since there is no demonstrable survival advantage for a 2-cm margin over a 1-cm margin in 1-mm to 2-mm melanomas:
- A 1-cm margin can be justified in cases in which a 2-cm margin is not easily achievable
- Based upon data from the WHO Trial and the Intergroup Melanoma Trial:
- A randomized prospective study conducted by the Intergroup Melanoma Committee compared 2-cm and 4-cm radial margins of excision for 1-mm to 4-mm thickness melanomas:
- Thick melanomas:
- The optimal margin width for thick melanomas (greater than 4 mm) is still unknown
- A retrospective review of 278 patients with thick primary melanomas from The University of Texas MD Anderson Cancer Center and Moffitt Cancer Center:
- Demonstrated that the width of the excision margin (≤ 2 cm vs. > 2 cm):
- Did not significantly affect local recurrence, disease-free survival, or OS rates after a median follow-up of 27 months
- Demonstrated that the width of the excision margin (≤ 2 cm vs. > 2 cm):
- In addition, based upon data from the UKMSG Trial:
- Investigators concluded that a 3-cm margin is better than 1-cm margin for melanomas 2 mm to 4 mm thick
- The Intergroup Melanoma Trial:
- 4-cm margin is not superior to a 2-cm margin for same tumor thickness):
- A margin greater than 2 cm is not necessary for these thick melanomas
- 4-cm margin is not superior to a 2-cm margin for same tumor thickness):

- Based in large part on the data from randomized, prospective trials, several recommendations can be made for margins of excision (Table):
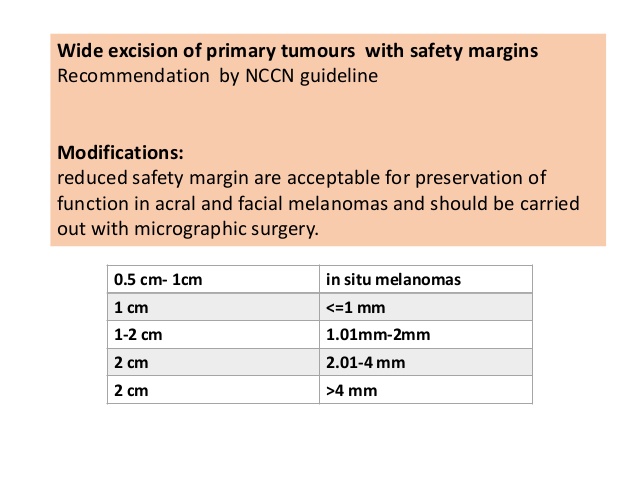
- Patient with melanoma in situ:
- A 0.5-cm to 1-cm margin is adequate
- Patients with invasive melanoma less than 1 mm thick:
- Can be treated with a 1-cm margin of excision
- Patients with melanoma 1 mm to 2 mm thick:
- A simple recommendation is difficult because this patient population has been studied in several trials evaluating a range of excision margins:
- In general, a 2-cm margin is preferred if anatomically and functionally feasible
-
- In regions of anatomical constraint (e.g., the face), a 1-cm margin is sufficient:
- This recommendation is based on the fact that OS was similar for patients with 1- and 3-cm margins in the WHO Trial
- In regions of anatomical constraint (e.g., the face), a 1-cm margin is sufficient:
- A simple recommendation is difficult because this patient population has been studied in several trials evaluating a range of excision margins:
- Patients with melanoma 2 mm to 4 mm thick:
- Can be treated with a 2-cm margin
- Patients with a melanoma thicker than 4 mm:
- A 2-cm margin is probably safe and is generally employed:
- Although no prospective randomized trials have specifically addressed this thickness group
- A 2-cm margin is probably safe and is generally employed:
Rodrigo Arrangoiz MS, MD, FACS
-
He is an expert in the management of skin cancer including MELANOMA
-
If you have any questions about the management of melanoma please fill free to contact Dr. Arrangoiz.
-
Article on Melanoma published by Dr. Arrangoiz:
-

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#HeadandNeckSurgeon
#CirujanodeTumoresdeCabezayCuello
#CancerSurgeon
#CirujanodeCancer
#MountSiniaMedicalCenter
#MSMC
