
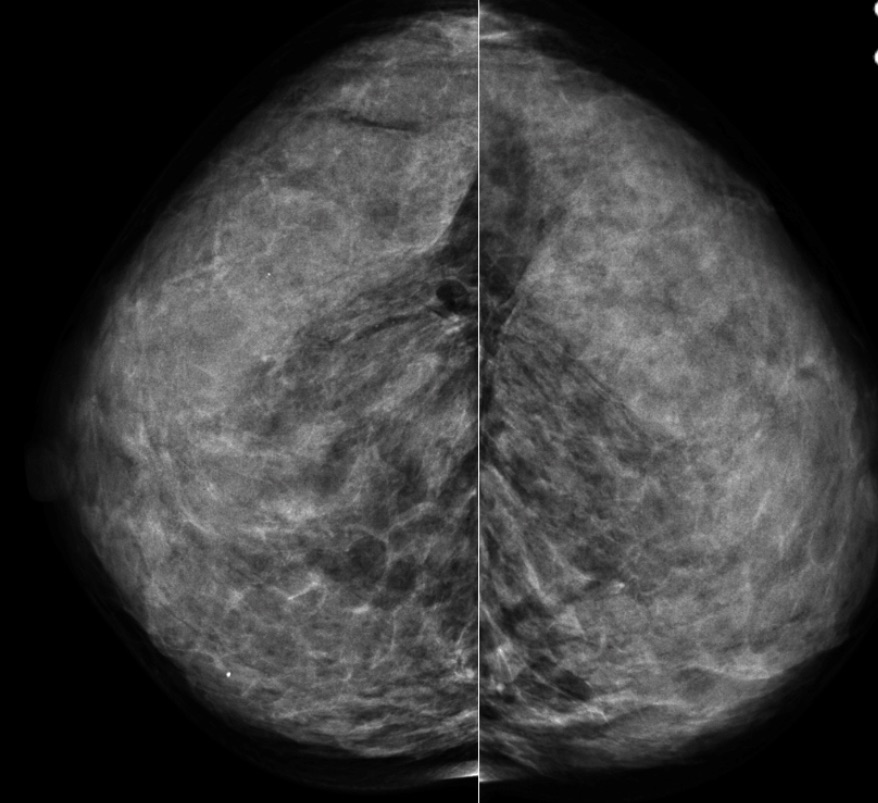
- The mammogram shows extremely dense breast tissue without other abnormality
- Because no particle movement could be identified, one cannot be certain the mass is not solid:
- If solid, the sonographic mass has none of the 10 signs of malignancy, but it also does not meet any of the 3 strict benign criteria:
- 10 signs of malignancy on ultrasound:
- Shadowing
- Hypoechoic ecotexutre
- Spiculation
- Angular Margins
- Thick echogenic halo
- Microlobulation
- Taller than wider
- Duct Extension
- Branching pattern
- Calcifications
- 10 signs of malignancy on ultrasound:
- The three benign findings defined by Stavros are:
- A purely hyperechoic lesion with no hypoechoic area larger than a normal duct or lobule
- Elliptical, wider than tall, well-circumscribed and thin echogenic capsule
- Gently lobulated, wider than tall, well-circumscribed and thin echogenic capsule
- If solid, the sonographic mass has none of the 10 signs of malignancy, but it also does not meet any of the 3 strict benign criteria:
- The ultrasound shows a round lesion that is neither elliptical nor gently lobulated, so even if a thin echogenic capsule could be identified, none of the 3 defined benign criteria are met:
- When there is a thin echogenic capsule in a solid lesion that does not meet the other criteria:
- There is a 14% chance of malignancy:
- Therefore, further evaluation is necessary
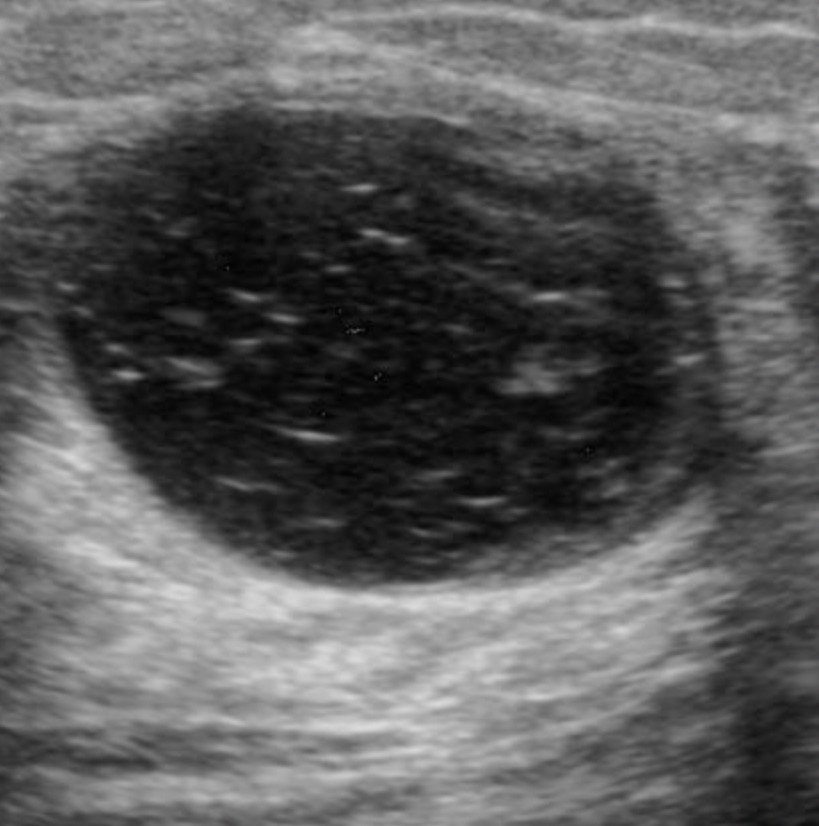
- Complicated cysts (Image):
- Differ from simple cysts:
- Only with regard to internal echoes
- Complicated cysts are circumscribed and show posterior acoustical enhancement:
- But are not anechoic
- They are old cysts that have gradually lost fluid through absorption:
- Leaving behind proteinaceous fluid, cholesterol crystals, blood, or other substances:
- That cause low-level internal echoes
- They can sometimes be difficult to distinguish from hypoechoic solid lesions
- If one can demonstrate swirling of particles within the mass either by “bouncing” the transducer against the lesion or increasing the power of the beam:
- The diagnosis of a cystic lesion can be made
- If there is no movement of particles:
- A solid mass cannot be excluded
- Although the lesion shown above would be considered BIRADS 3 by many radiologists, and 6-month follow-up would perhaps be recommended, that approach might cause unnecessary anxiety:
- There would also be the possibility of diagnostic delay if the lesion turned out to be a well-circumscribed cancer
- For these reasons, the best approach is to aspirate the lesion and try to evacuate the fluid:
- Sometimes the “fluid” is the consistency of toothpaste and requires a 16- or even 14-gauge needle to evacuate it:
- If nothing is obtained with a large bore needle, core needle biopsy is indicated
- Sometimes the “fluid” is the consistency of toothpaste and requires a 16- or even 14-gauge needle to evacuate it:
- Leaving behind proteinaceous fluid, cholesterol crystals, blood, or other substances:
- Differ from simple cysts:
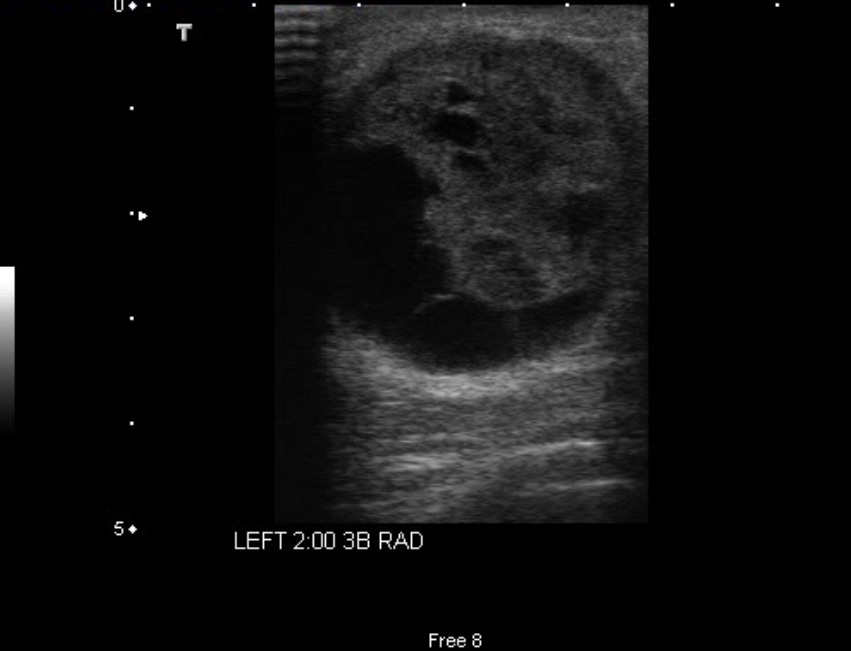

- A “complex” cyst:
- Has both cystic and solid components (Images)
- The solid component may take the form of:
- An intracystic mass or a thickened septum with a convex component
- Biopsy is indicated to establish the diagnosis
- If the lesion is large enough, biopsy can usually be obtained with a core device without vacuum assistance
- If the lesion is predominately cystic with a thickened, convex septum:
- Percutaneous vacuum-assisted or surgical excision may be required because the lesion may not be visible after initial core needle targeting, resulting in incomplete sampling
- Vacuum-assisted sampling is usually adequate to establish a diagnosis and plan surgical therapy, if needed
- On the other hand, surgical excision of either of these complex cysts would give the pathologist the advantage of examining the entire specimen intact
- References
- D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas: Breast Imaging Reporting and Data System, 5th ed. Reston, VA: American College of Radiology; 2013.
- Berg WA, Sechtin AC, Marques H, Zhang Z. Cystic breast masses and the ACRIN 666 experience. Radiol Clin North Am. 2010;48(5):931-987.
- Stavros AT. Sonographic evaluation of breast cysts. In: Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004:276-350.

