- Radiation techniques for DCIS – Hypofractionation
- ASTRO evidence-based guideline from 2018:
- Stage (including DCIS vs invasive breast cancer):
- Statement KQ1G:
- Hypofractionation whole breast irradiation (WBI) may be used as an alternative to conventional fractionation (CF) CF-WBE in patients with DCIS
- Recommendation strength: conditional
- Quality of evidence: Moderate
- Consensus: 86%
- Hypofractionation whole breast irradiation (WBI) may be used as an alternative to conventional fractionation (CF) CF-WBE in patients with DCIS
- Statement KQ1G:
- Age, grade, and margins for DCIS:
- Statement KQ2D:
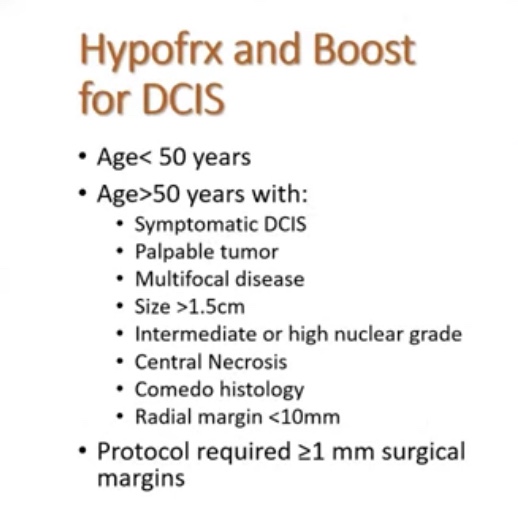
- A tumor boost may be used for patients with DCIS who meet any of the following criteria:
- Age =/< 50 years
- High grade
- Close (< 2 mm) or positive margins
- Recommendation strength: conditional
- Quality of evidence: Moderate
- Consensus: 92%
- A tumor boost may be used for patients with DCIS who meet any of the following criteria:
- Statement KQ2D:
- Stage (including DCIS vs invasive breast cancer):
- ASTRO evidence-based guideline from 2018:
- This two statements from ASTRO rely of data from two randomized trials:
- The DBCG Hypo Trial:
- Entry criteria:
- > 40 years of age
- BCS for node-negative breast cancer
- DCIS (13% of the cohort)
- Primary endpoint:
- Grade 2 to 3 breast induration assuming no inferiority regarding locoregional recurrence
- Median follow-up of 7.26 years
- Entry criteria:
- The DBCG Hypo Trial:


- BIG 3-07 / TROG 07.01:
- Background:
- Whole breast irradiation (WBI) after conservative surgery for ductal carcinoma in situ (DCIS) reduces local recurrence.
- They investigated whether a tumor bed boost after WBI improved outcomes, and examined radiation dose fractionation sensitivity for non-low-risk DCIS.
- Methods:
- The study was an international, randomized, unmasked, phase 3 trial involving 136 participating centres of six clinical trials organisations in 11 countries (Australia, New Zealand, Singapore, Canada, the Netherlands, Belgium, France, Switzerland, Italy, Ireland, and the UK).
- Eligible patients were women aged 18 years or older with unilateral, histologically proven, non-low-risk DCIS treated by breast-conserving surgery with at least 1 mm of clear radial resection margins.
- They were assigned to one of four groups (1:1:1:1) of no tumour bed boost versus boost after conventional versus hypofractionated WBI, or randomly assigned to one of two groups (1:1) of no boost versus boost after each center prespecified conventional or hypofractionated WBI.
- The conventional WBI used was 50 Gy in 25 fractions, and hypofractionated WBI was 42.5 Gy in 16 fractions. A boost dose of 16 Gy in eight fractions, if allocated, was delivered after WBI.
- Patients and clinicians were not masked to treatment allocation. The primary endpoint was time to local recurrence.
- Findings:
- Between June 25, 2007, and June 30, 2014, 1608 patients were randomly assigned to have no boost (805 patients) or boost (803 patients).
- Conventional WBI was given to 831 patients, and hypofractionated WBI was given to 777 patients.
- Median follow-up was 6.6 years.
- The 5-year free-from-local-recurrence rates were 92.7% (95% CI 90·6-94·4%) in the no-boost group and 97.1% (95·6-98·1%) in the boost group (hazard ratio 0·47; 0·31-0·72; p<0·001).
- The boost group had higher rates of grade 2 or higher breast pain (10% [8-12%] vs 14% [12-17%], p=0·003) and induration (6% [5-8%] vs 14% [11-16%], p<0·001).
- Interpretation:
- In patients with resected non-low-risk DCIS, a tumor bed boost after WBI reduced local recurrence with an increase in grade 2 or greater toxicity.
- The results provide the first randomised trial data to support the use of boost radiation after postoperative WBI in these patients to improve local control.
- The international scale of the study supports the generalizability of the results.
- Background:
- Radiation Techniques for DCIS:
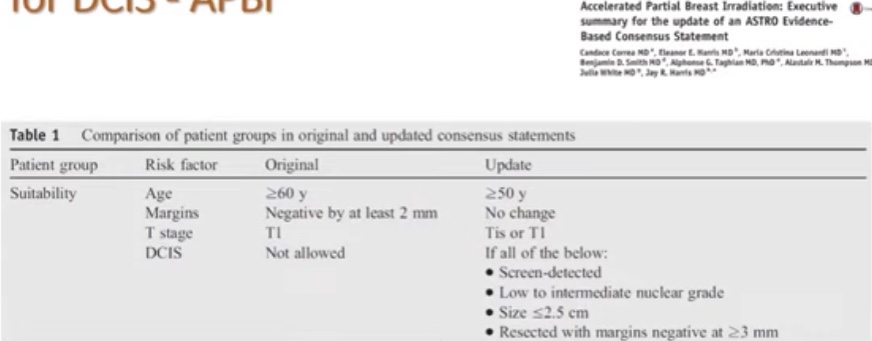
- Accelerated partial breast irradiation:
- Summary:
- Moderately hypo-fractionation WBI is a standard treatment
- Consider boost for:
- High grade DCIS
- > 2 cm tumors
- Positive or < 2 mm margins
- Pre-menopausal patients
- Patients less than 50 years of age
- APBI in DCIS is safe and effective option in ASTRO “suitable”candidates
- Not all techniques (just validated with external beam radiation)
- Consider hormone therapy in aggressively minded patients or those wishing to decrease risk of contralateral breast cancer
- Consider genomic assay assistance to aid in radiation decisions in select patients:
- Postmenopausal patients with otherwise low-risk disease

