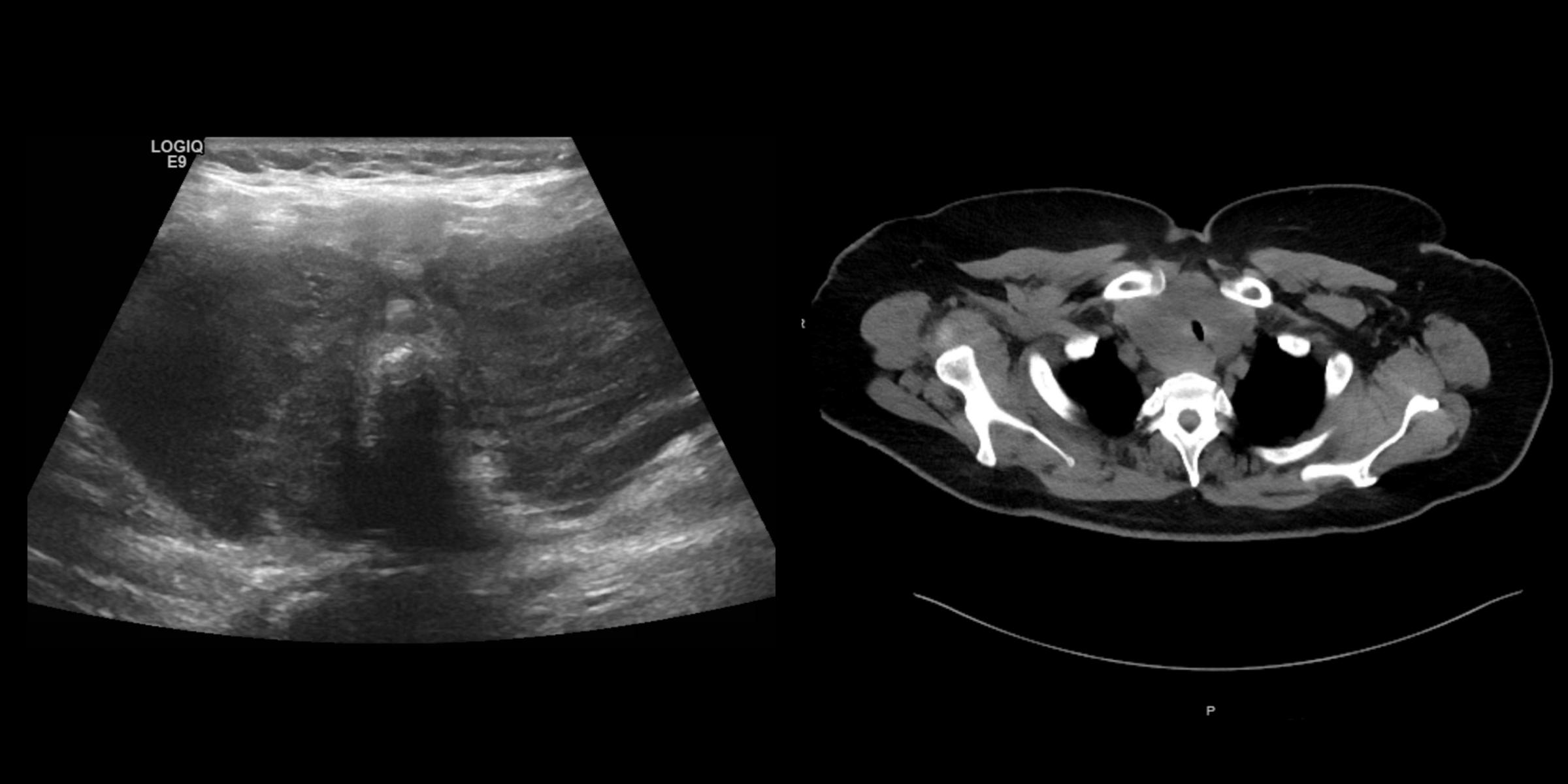
A 61-year-old woman presented to the hospital with dysphagia to solid foods and dyspnea on exertion that has been worsening over the last 1-2 months. Past medical history includes hypothyroidism from Hashimoto’s thyroiditis on levothyroxine, and T2DM on metformin (well-controlled). Physical exam is notable for significant diffuse thyroid enlargement, not rock hard or tender thyroid, positive Pemberton’s sign, hoarse voice (but she is able to speak in full sentences). Biochemical testing revealed normal CBC, CMP, and a TSH of 5.02 uIU/mL (normal 0.5-5.7). Thyroid ultrasound and neck CT are shown below.
What Is the Most Likely Cause for This Finding?
- Anaplastic thyroid carcinoma
- Fibrous thyroiditis
- Subacute thyroiditis
- Diffuse large B-cell lymphoma
- Mucosa-associated lymphoid tissue (MALT) lymphoma
Correct Answer: Diffuse large B-cell lymphoma
This patient, with a history of Hashimoto’s thyroiditis, presents with a rapidly enlarging thyroid mass that has caused dysphagia and dyspnea on exertion. In that clinical context, the most likely etiology of her symptoms is thyroid lymphoma, and the most common type of primary thyroid lymphoma is diffuse large B-cell lymphoma (DLBCL). Thyroid lymphoma is a rare malignancy representing less than 5% of all thyroid cancers. Hashimoto’s thyroiditis is a well-established risk factor, as patients with Hashimoto’s thyroiditis have a 60 times higher risk of developing primary thyroid lymphoma, compared to the general population. On ultrasound, thyroid lymphoma will appear with diffuse enlargement of the thyroid in a uniform and very hypoechoic pattern, like the one presented here. Usually cross-sectional imaging will be needed, and in this case, there was the apparent narrowing of the upper trachea.
DLBCL usually appears malignant on cytology, while MALT lymphoma can be more subtle, which might result in an Atypia of Undetermined Significance (AUS) by the Bethesda classification. If lymphoma is clinically suspected, it is very important to obtain material for flow cytometry with the biopsy. Treatment of thyroid lymphomas depends on the subtype and staging of the tumor. Usually R-CHOP (rituximab- cyclophosphamide, doxorubicin, vincristine, prednisolone) is used, and no thyroidectomy is recommended.
This patient did not appear to demonstrate hyperthyroidism, nor had a tender thyroid gland, so subacute thyroiditis is unlikely. Fibrous thyroiditis (or Riedel’s thyroiditis) will present with a very hard, fixed goiter. Anaplastic thyroid carcinoma would usually present with asymmetric enlargement of the thyroid, as there is usually a dominant nodule that does not involve the thyroid gland in its entirety

