- Two Strategies of Ventilation:
- Injury:
- This strategy is for patients with lung injury and those prone to lung injury
- Essentially this means every intubated patient:
- Except those with obstruction
- Essentially this means every intubated patient:
- This strategy is for patients with lung injury and those prone to lung injury
- Obstruction:
- Use this strategy when patients are in the midst of an Asthma / COPD exacerbation
- Injury:
- Injury Strategy:
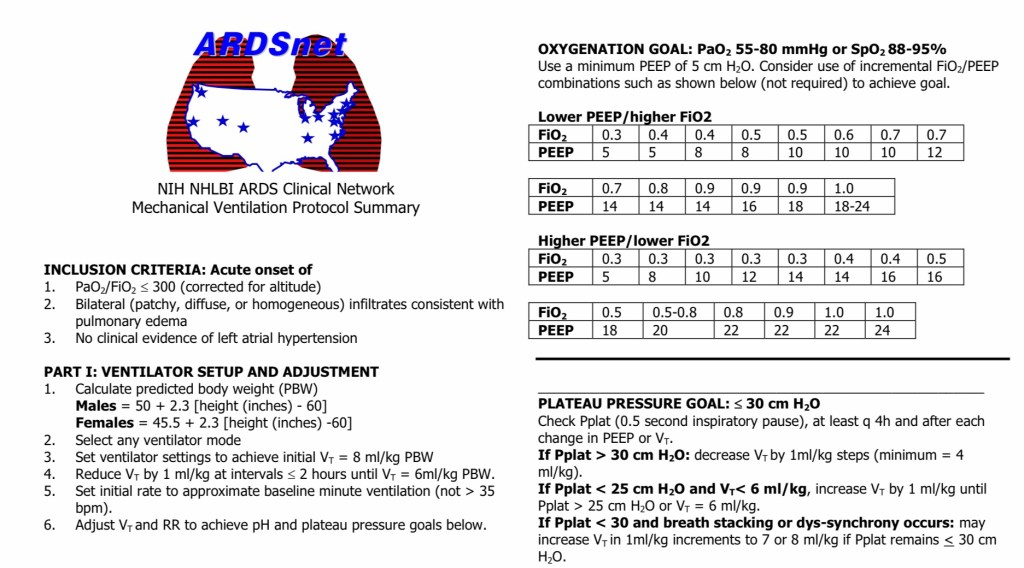
- Based on ARDSnet:
- ARMA Study:
- N Engl J Med 2000;342,1301-1308
- ARMA Study:
- Mode:
- Assist Control (AC)-Volume
- Tidal Volume (Vt):
- Equals:
- Protection
- Start at 6 to 8 ml / kg:
- Based on PBW
- If ALI / ARDS:
- The goal is to get down to 6 mo / kg:
- Why?
- Injured lungs are baby lungs
- Why?
- The goal is to get down to 6 mo / kg:
- This setting should not be altered:
- To fix ventilation
- It only gets changed:
- For lung protection/
- To prevent:
- Barotrauma / volutrauma
- To prevent:
- For lung protection/
- Equals:
- Flow Rate (IFR):
- Equals:
- Comfort
- Start at 60 to 80 liters per minute (lpm)
- This setting controls:
- How quickly the air goes in
- Equals:
- Rate (RR):
- Equals:
- Ventilation
- Initially start at 16 to 18 breaths per minute (bpm):
- Adjust based on:
- CO2 and ventilatory needs
- Adjust based on:
- Alveolar gas volume (Va):
- For maintaining normal CO2 when not intubated:
- Is 60 ml /kg / min
- We need to double that:
- To 120 cc/kg/min:
- When intubated because of:
- Increased deadspace:
- Need double that volume (240 ml /kg / min) to send CO2 from 40 to 30
- Increased deadspace:
- When intubated because of:
- To 120 cc/kg/min:
- Try to keep mildly hypercarbic
- For maintaining normal CO2 when not intubated:
- Equals:
- FiO2/PEEP:
- Equals:
- Oxygenation
- Start at:
- 100% FiO2 and PEEP of 5
- Wait 5 minutes:
- Then draw an ABG
- Then set the FiO2 between 30% to 40%:
- Start titrating:
- Based on the ARDS Net protocol chart:
- Go up every 5 to 10 minutes:
- Quicker if low saturation
- Quicker if low saturation
- Start titrating:
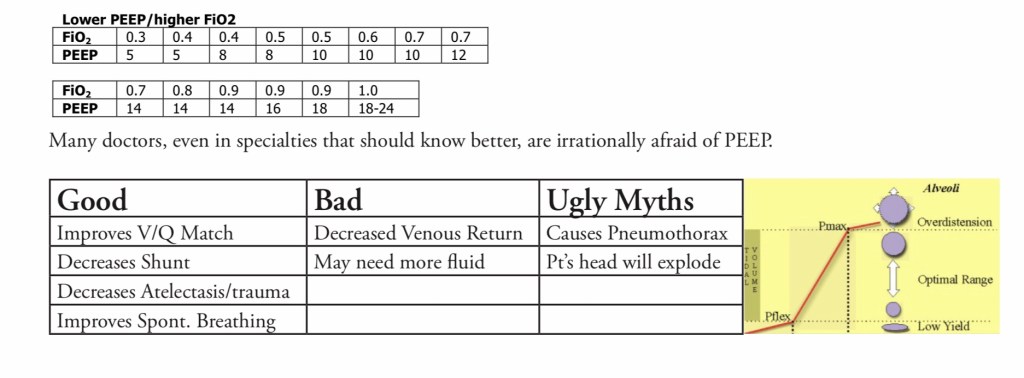
- Oxygenation goal:
- PaO2 between:
- 55 mmHg to 80 mmHg
- SpO2 between:
- 88% to 95%
- PaO2 between:
- Use a minimum PEEP of:
- 5 cm H2O
- Consider use of incremental FiO2 / PEEP combinations such as shown below to achieve goal:
- Equals:
- Based on ARDSnet:
- Check Plateau Pressure:
- Check it after:
- Initial settings and at regular intervals thereafter
- Use the inspiratory hold button:
- Hold for 0.5 seconds:
- Look at pressure gauge
- Hold for 0.5 seconds:
- The peak pressure:
- Is essentially meaningless
- Plateau pressure:
- Must be maintained less than 30 cm H20
- Keep lowering the tidal volume (Vt):
- Until Plat less than 30 cm H20:
- You may need to go as low as 4 ml / kg
- Until Plat less than 30 cm H20:
- Disadvantages of this strategy:
- It is not the most comfortable strategy of ventilation for awake, spontaneously breathing patients:
- Use sedation / pain medications
- Give enough flow:
- If you see the patient sucking the straw:
- Increase the IFR setting
- If you see the patient sucking the straw:
- It is not the most comfortable strategy of ventilation for awake, spontaneously breathing patients:
- Check it after:
- Obstructive Strategy:
- Goal is to:
- Give as much expiratory time as possible
- Mode:
- Assist Control
- Vt:
- 8 ml / kg by PBW
- IFR:
- 80 to 100 lpm
- PEEP:
- 0 to 5 cmH20
- FiO2:
- Use whatever you need:
- Most use 40%
- Use whatever you need:
- RR:
- Start at 8 to 10 bpm:
- Look for:
- I:E of 1:4 or 1:5:
- Adjust the rate to achieve this
- I:E of 1:4 or 1:5:
- Look for:
- Start at 8 to 10 bpm:
- Goal is to:
- Permissive Hypercapnia:
- Patients will need a lot of sedation / opioids
- Keep pH above:
- 7.1:
- Rarely:
- You may need a bicarbonate drip to accomplish this
- Rarely:
- 7.1:
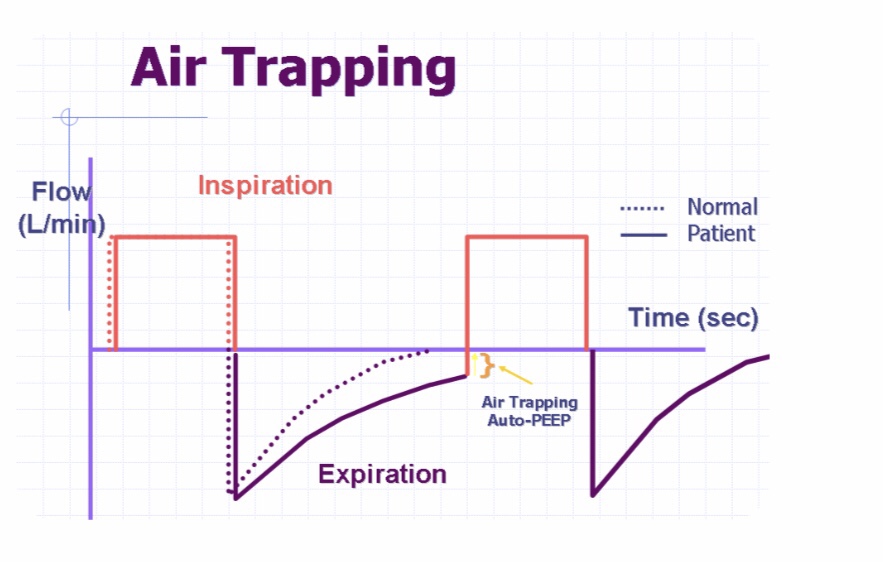
- AutoPEEP and Airtrapping:
- They decrease venous return
- Impede expiration
- Impede spontaneous ventilation
- Other Concerns:
- Large Tubes:
- At least size 8.0 ET whenever possible:
- For both male and female patients.
- Pulmonary toilet and ICU care:
- Is miserable with small tubes
- Biofilm forms:
- Within the first two days reducing tube size dramatically
- At least size 8.0 ET whenever possible:
- Large Tubes:
- Ventilator Alarms:
- Treat them like a code announcement:
- The closest person should run to the patients bedside and assess the situation.
- Treat them like a code announcement:
#Arrangoiz #Teacher #Surgeon
