- According to Brigham and Women’s Hospital COVID-19 Critical Care Clinical Guidelines:
- Patients with COVID-19 generally present with respiratory symptoms:
- More specifically:
- Cough:
- 46% to 82% of the cases
- Shortness of breath:
- 20% to 64% of the cases
- Upper respiratory tract symptoms:
- 5% to 25% of the cases:
- Including nasal / sinus congestion
- 5% to 25% of the cases:
- Cough:
- More specifically:
- Patients with COVID-19 generally present with respiratory symptoms:
- The Brigham and Women’s Hospital guidelines further state that:
- Approximately 20% of those with COVID-19 develop ARDS
- 2% to 25% have a respiratory viral co-infection
- The most common cause of ICU admission for COVID-19 patients is:
- Hypoxemic respiratory failure
- Among those admitted:
- Intubation is often required within 12 to 24 hours
- Of COVID-19 patients who die:
- About half die from respiratory failure
- Third die from concomitant respiratory and heart failure
- Many patients with COVID-19 are presenting with:
- Hypoxemia disproportionate:
- To their imaging findings
- Hypoxemia disproportionate:
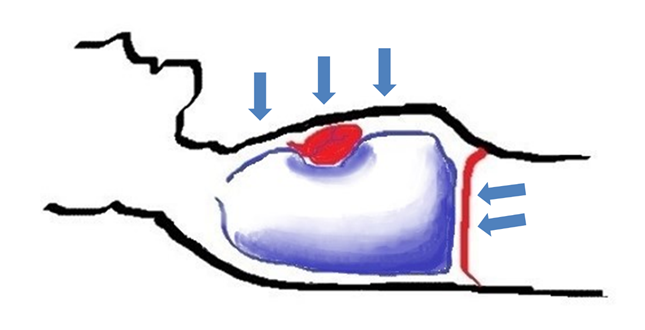
- Hypoxemia arises in ARDS:
- Through a mismatch of ventilation and perfusion:
- Predominantly due to shunt:
- 1 to 3 with shunt fractions much greater than would be anticipated for their relatively compliant lungs
- Predominantly due to shunt:
- Through a mismatch of ventilation and perfusion:
- Patients with COVID-19 have:
- Scattered, peripheral ground glass opacities on chest computed tomography scans:
- Indicating ineffective lung units, and as such:
- Shunt:
- Appears to be a major cause of the hypoxemia
- Shunt:
- Indicating ineffective lung units, and as such:
- Dr. Gattioni and colleagues report:
- Disproportionate blood flow to these areas:
- Possibly accounting for the profound hypoxemia
- They suggest at least two distinct phenotypes:
- Low recruitability phenotype:
- Presenting with:
- Low elastance
- High compliance
- Low recruitability
- But yet substantial hypoxemia:
- They hypothesis that a mechanism for this profound hypoxemia could be:
- Loss of V/Q matching from:
- Pulmonary arterial vasoplegia
- Loss of V/Q matching from:
- They hypothesis that a mechanism for this profound hypoxemia could be:
- But yet substantial hypoxemia:
- Presenting with:
- Low recruitability phenotype:
- Later, patients progressed to the H phenotype:
- High elastance
- Low compliance
- High recruitability
- Need for higher PEEP
- Disproportionate blood flow to these areas:
- Scattered, peripheral ground glass opacities on chest computed tomography scans:
- The CT scan below demonstrates the mild-moderate ground glass findings in COVID-19:
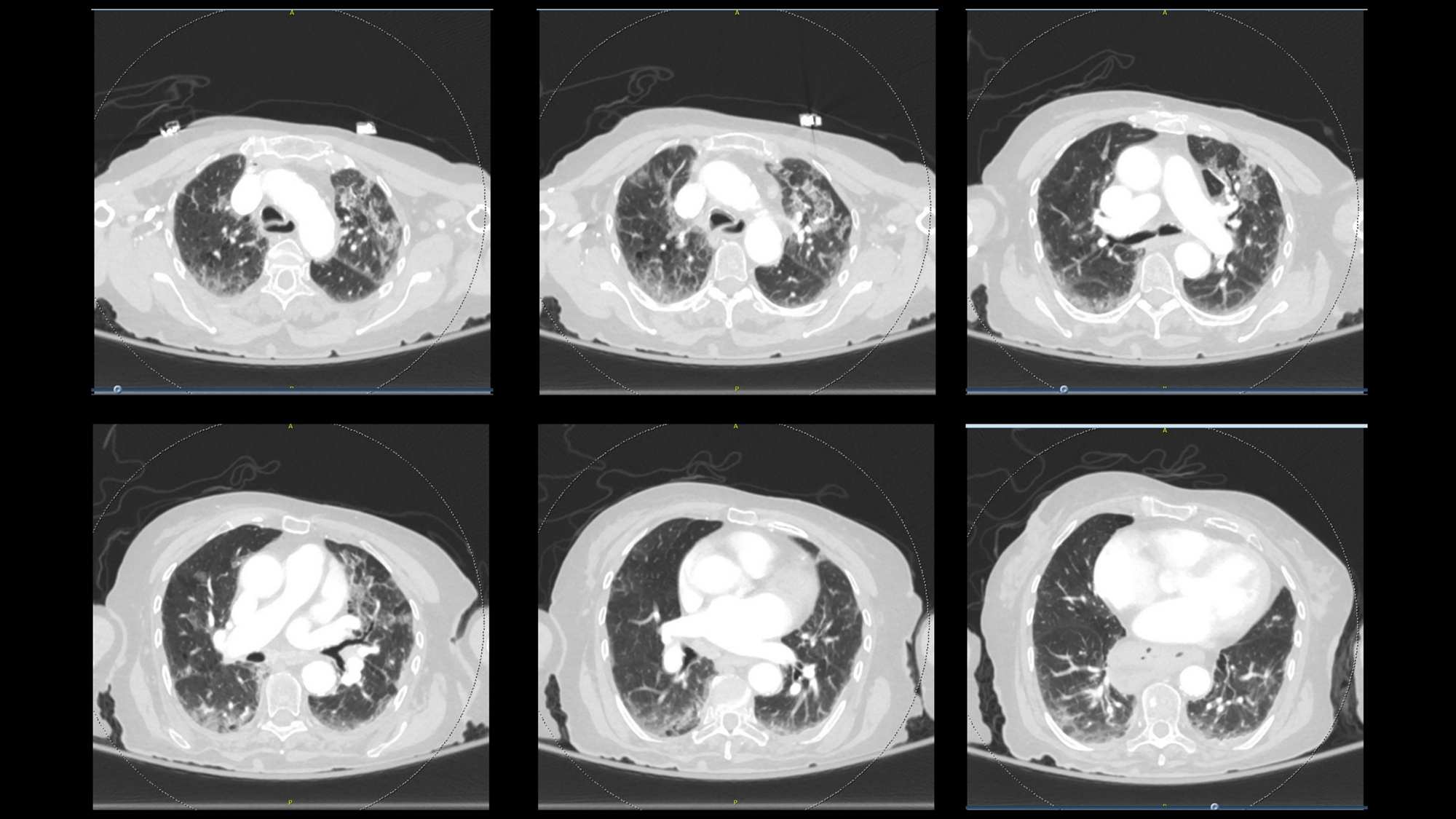
- On presentation:
- Patients are presenting with substantial hypoxemia:
- With many having oxygen saturations in the 70s, 80s, 90s:
- They deteriorate with any exertion
- With many having oxygen saturations in the 70s, 80s, 90s:
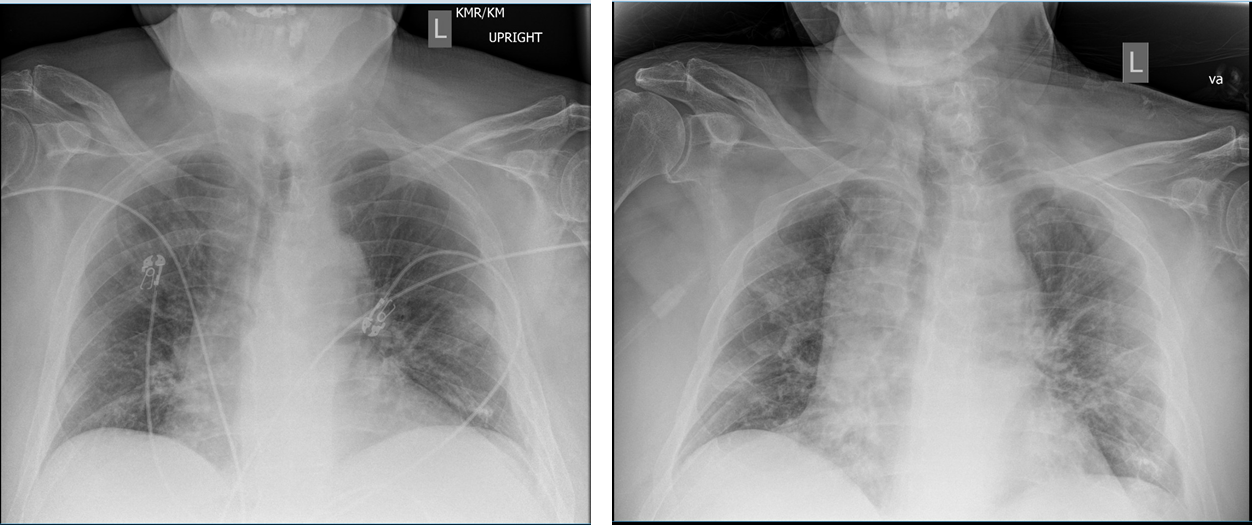
- Chest x-ray imaging will vary substantially depending upon where the patient is in the course of their illness
- Patients are presenting with substantial hypoxemia:
- The initial mode of treatment involves:
- Providing supplemental oxygen immediately to improve the oxygen saturation
- Although patients may or may not be complaining of dyspnea:
- Nearly all hypoxemic patients are noted to be tachypneic:
- Patients who are tachypneic:
- Generate large tidal volumes:
- Which can induce lung injury:
- From generating large negative intrathoracic pressure and therefore a large transpulmonary pressure
- Which can induce lung injury:
- Generate large tidal volumes:
- As such, the hypoxemia should be treated to:
- Decrease hypoxemic drive
- Patients who are tachypneic:
- Nearly all hypoxemic patients are noted to be tachypneic:
- The role of high-flow nasal cannula and non-invasive positive pressure ventilation:
- Are controversial in COVID-19:
- The concerns are for healthcare workers, as the risk of aerosolization has been noted with these modalities, especially non-invasive positive pressure ventilation
- Although there are limited data regarding the use of HNFC in COVID-19:
- A small study of patients with Influenza A showed that 45% avoided intubation:
- Although all more severe patients were eventually intubated
- A small study of patients with Influenza A showed that 45% avoided intubation:
- Are controversial in COVID-19:
- Similarly, non-invasive positive pressure ventilation (NIPPV) is a common means of respiratory support in many patients:
- But its use in COVID-19 should be limited
- NIPPV failed in 57% to 85% of patients with Influenza A H1N1 associated ARDS:
- With failing patients having a higher ICU mortality than those treated with invasive mechanical ventilation
- Some component of this may be due to patients continuing to:
- Generate those large tidal volumes
- Continuing to induce self-inflicted lung injury
- Subjects with SOFA score ≥ 5 had a higher risk of NIV failure (odds ratio = 3.3, 95% CI 2.4-4.5)
- A small study of COVID-19 patients in Wuhan found that 76% failed NIPPV, and the mortality rates were similarly high for both groups
- NIPPV also aerosolizes the virus:
- Many recommend that it should be avoided in most circumstances:
- However, there may well be a role for judicious use of non-invasive ventilation in COVID-19
- Each institution is developing their own policies and procedures, with some adopting the process widely and others not using it at all
- Many recommend that it should be avoided in most circumstances:
- When the decision is made to intubate a patient:
- The patient can have significant clinical deterioration with COVID-19
- The patient arrives with a high work of breathing:
- Generating substantial negative intrathoracic pressure:
- To maintain minute ventilation and V/Q matching
- Generating substantial negative intrathoracic pressure:
- When the patient is intubated:
- The induction agents and paralytics are administered, the patient is laid in a recumbent position, and the patient will be derecruited
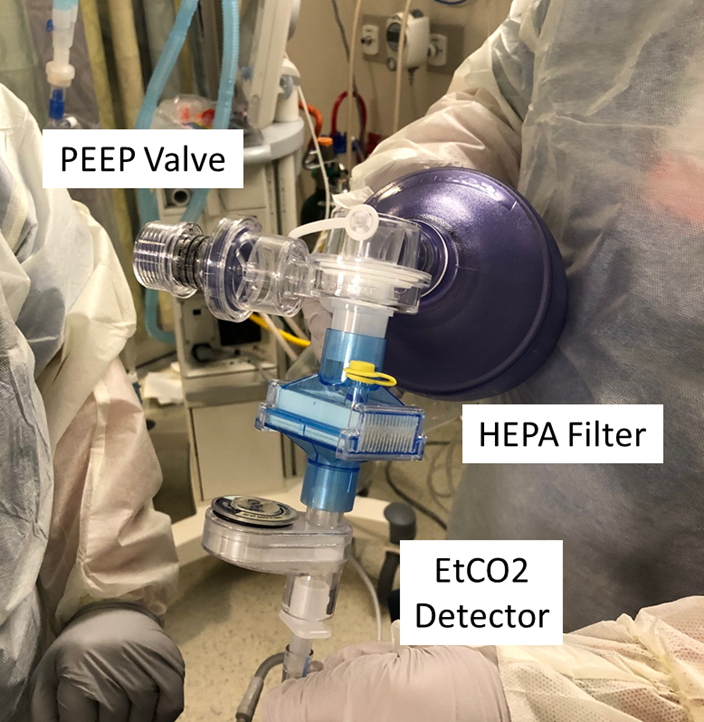
- Recruiting the patient can be a substantial endeavor:
- Typically, we use a bag method with a PEEP valve to recruit patients and prepare them to be placed on the ventilator immediately after intubation:
- If this method is to be used, a HEPA filter must be placed between the endotracheal tube and the bag:
- However, many institutions are now foregoing any bagging and instead placing the patient directly on the ventilator:
- To reduce the risk of aerosolization
- An advantage is:
- That the patient does not receive any:
- High tidal volume, high-pressure breaths from the bagging
- That the patient does not receive any:
- The downside, however, is:
- That recruitment may take longer, and these patients may be profoundly hypoxemic during that time period
- However, many institutions are now foregoing any bagging and instead placing the patient directly on the ventilator:
- If this method is to be used, a HEPA filter must be placed between the endotracheal tube and the bag:
- Typically, we use a bag method with a PEEP valve to recruit patients and prepare them to be placed on the ventilator immediately after intubation:
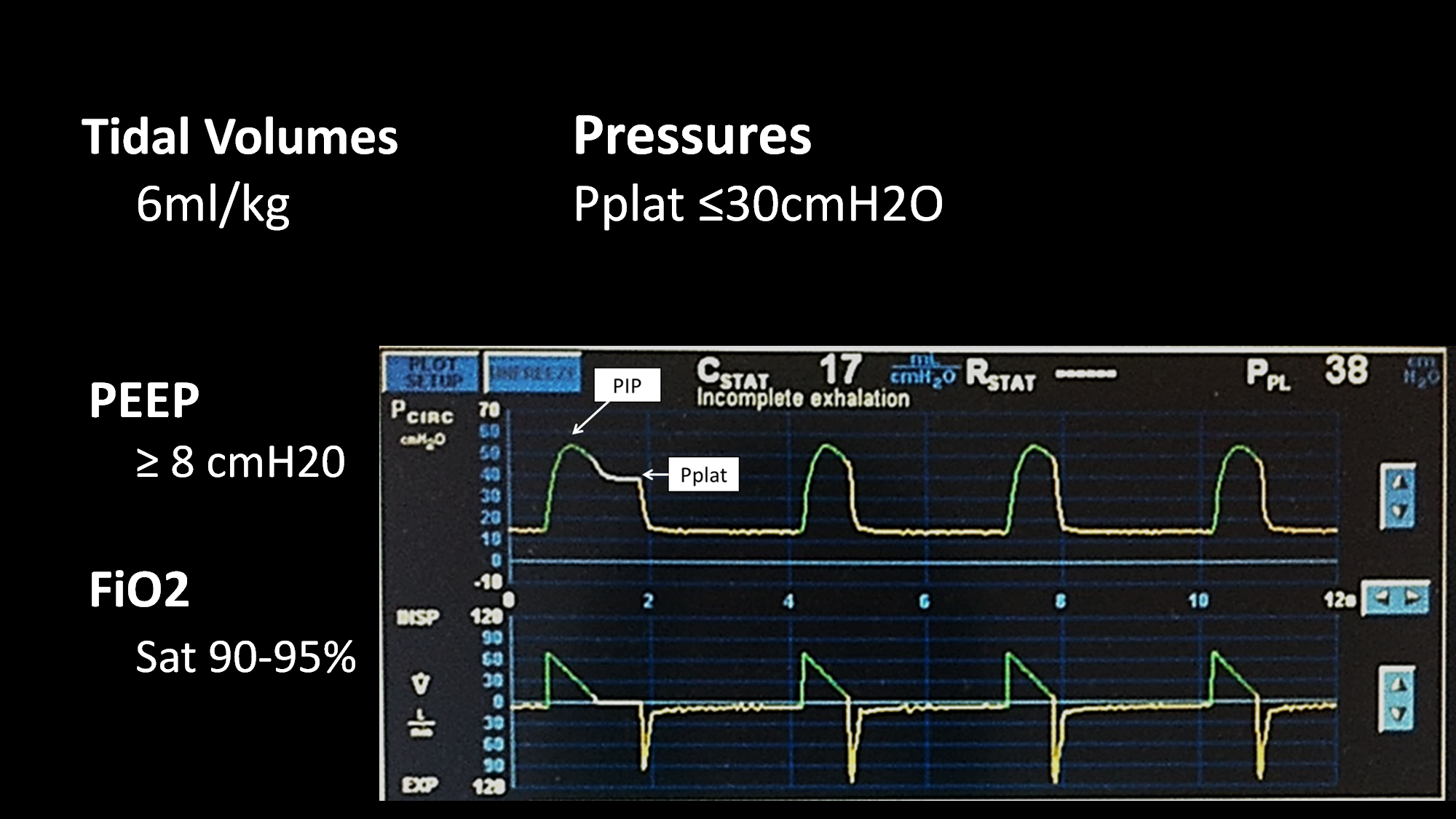
- Once the patient is placed on the ventilator, general principles of good ventilator management still apply:
- The patient should be placed on:
- Low tidal volume ventilation:
- 4 ml/kg to 8 ml/kg of PBW:
- Starting with a tidal volume of 6 ml/kg of predicted body weight
- 4 ml/kg to 8 ml/kg of PBW:
- The plateau pressure should be checked and monitored:
- Ensuring a value less than 30 cm of water
- The driving pressure should be:
- Less than 15 centimeters of water
- These patients likely require a moderate PEEP at least:
- We recommend starting with a PEEP of 8 and adjusting from there:
- While PEEP can improve oxygenation:
- Too much PEEP can be deleterious causing:
- Increased intrathoracic pressure
- Lung injury
- Hemodynamic compromise if severe
- Too much PEEP can be deleterious causing:
- While PEEP can improve oxygenation:
- We recommend starting with a PEEP of 8 and adjusting from there:
- Low tidal volume ventilation:
- The patient should be placed on:
- For patients with COVID-19:
- Who have a PaO2 / FiO2 ratio of less than a 150:
- The next step should be placing the patient:
- In a prone position:
- Many institutions have protocols or guidelines for prone positioning
- Prone positioning has been shown to improve mortality in patients with ARDS:
- Authors are reporting good outcomes with proning in patients with COVID-19
- Although a simple procedure, it requires a systems-based approach, with investment from nurses, respiratory therapists, and physicians alike
- All attention must be on the patient’s endotracheal tube, invasive lines, and position during the turns
- Additionally, close attention must be paid to patients in a prone position to ensure that their orbits and eyes are protected, that pressure points are well-supported, that medical equipment is not trapped under the body, possibly causing opportunity for injury or bedsores
- Most protocols involve:
- Leaving the patient in the prone position for 12 to 16 hours
- The patient will be reproned as long as their PaO2/ Fi02 ratio remains:
- Less than 150 while they are supine
- When the patient’s PaO2/ FiO2 ratio starts to improve:
- The patient no longer requires routine proning
- The next step should be placing the patient:
- Who have a PaO2 / FiO2 ratio of less than a 150:
- For patients with persistent severe hypoxemia:
- Inhaled pulmonary vasodilators:
- Can be considered
- Inhaled epoprostenol is an excellent pulmonary vasodilator:
- However, it is not recommended in COVID-19 as it mandates frequent ventilator circuit changes
- Therefore, if an inhaled pulmonary vasodilator is needed:
- Inhaled nitric oxide is preferred:
- We start at 20 parts per million and assess the patient for an improvement in SpO2
- If the patient does not have at least a 20% improvement in the SpO2:
- The inhaled pulmonary vasodilator is unlikely to be effective and should not be continued
- If the patient is responsive, the pulmonary vasodilator can be continued with gradual weaning as a patient improves clinically over the next several days
- Inhaled nitric oxide is preferred:
- Inhaled pulmonary vasodilators:
- Bacterial superinfection:
- Has been noted in about 20% to 30% of patients with COVID-19, and as such:
- Many patients will require antibiotics
- Procalcitonin can be useful for assessing COVID-19 alone
- Has been noted in about 20% to 30% of patients with COVID-19, and as such:
- Steroids are not routinely recommended for COVID-19 treatment:
- However, patients who have another indication for steroids:
- Such as asthma or adrenal insufficiency:
- They should receive them
- Such as asthma or adrenal insufficiency:
- The surviving sepsis campaign recommends use of steroids in severe ARDS:
- However, this is not a universal recommendation
- However, patients who have another indication for steroids:
- The role of other medications including:
- Hydroxychloroquine, azithromycin, and statins:
- Are unclear
- We encourage everyone to refer to local protocols for guidance on the use of these medications
- Some medications, such as Remdesivir, are being evaluated in clinical trials
- Hydroxychloroquine, azithromycin, and statins:
- Although CT scans:
- Have been shown to be fairly sensitive for the diagnosis of COVID-19:
- Once the diagnosis is made:
- We do not encourage the routine use of CT scans:
- Not only does a CT scan pose risk to a critically ill patient, mandating travel with the associated risks of line pulls, hemodynamic instability, and hypoxemia, but this can lead to infection control issues mandating the cleaning of the scanners as well
- We do not encourage the routine use of CT scans:
- Once the diagnosis is made:
- Have been shown to be fairly sensitive for the diagnosis of COVID-19:
- Patients with COVID-19:
- Have been noted to be fairly hypercoagulable:
- With many authors reporting:
- Thromboembolic disease, clotting of dialysis lines, and other clinical manifestations of hypercoagulability:
- D-dimer levels can be quite elevated coming into the thousands
- Thromboembolic disease, clotting of dialysis lines, and other clinical manifestations of hypercoagulability:
- The best practices for initiation of therapeutic anticoagulation:
- In the absence of a documented thromboembolism:
- Are unclear at this time:
- Some clinicians are using markedly elevated D-dimer levels:
- Such as greater than 2000:
- As an indication for anticoagulation, whereas others are basing it upon clotting of lines and other clinical markers
- Such as greater than 2000:
- Some clinicians are using markedly elevated D-dimer levels:
- Are unclear at this time:
- In the absence of a documented thromboembolism:
- With many authors reporting:
- Have been noted to be fairly hypercoagulable:
- Bronchoscopy is an aerosolizing procedure and as such:
- Should be minimized or avoided in patients with COVID-19
- Additionally, suctioning can be aerosolizing and all healthcare workers in the room should be aware and in appropriate PPE before these procedures are performed
#Arrangoiz #Teacher #Surgeon
