👉The nasopharynx is a difficult area to access surgically due to:
- Its central location
- Its surrounding facial skeleton and skull base
- Presence of great vessels and lower cranial nerves
👉The ideal surgical approach to the nasopharynx should:
- Provide adequate exposure to the nasopharynx:
- For tumor resection
- The great vessels:
- Must be safely controlled
- Lower cranial nerves:
- Should be spared
👉The surgical approach chosen is dependent on:
- Extent of primary tumor (size / T stage)
- Surgical expertise
- Facilities available
👉Classification of the surgical approaches to the nasopharynx:
- Anterior approach
- Inferior approach
- Lateral approach
👉Anterior approaches to the nasopharynx:
- Lateral rhinotomy
- Transnasal transmaxillary approach
- Midfacial degloving
- Lefort I osteotomy
- Maxillary swing approach
👉Lateral rhinotomy:
- This approach exposes the:
- Nasal cavity and choana well
- It can be used alone or in combination with other surgical approaches:
- To enhance exposure of the nasopharynx
- This approach is useful in resection of:
- Anteriorly placed tumors
👉Transnasal transmaxillary approach:
- In this approach a lateral rhinotomy is combined with:
- A medial / subtotal maxillectomy
- This approach exposes the:
- Nasopharynx
- Ipsilateral spheno-ethmoidal complex
- Pterygopalatine fossa
- Medial end of infratemporal fossa
👉Midfacial degloving approach:
- This is a bilateral transnasal, transmaxillary approach
- The advantage of this procedure is that it is performed:
- Via sublabial incision:
- Thereby avoiding facial scar
- Via sublabial incision:
- In this approach the:
- Infraorbital nerves on both sides:
- Are safeguarded
- Midface is degloved subperiosteally:
- Up to the level of root of the nose
- A bilateral medial maxillectomy is performed to improve exposure
- The pterygopalatine fossa and the medial end of infratemporal fossa is ideally exposed
- Infraorbital nerves on both sides:
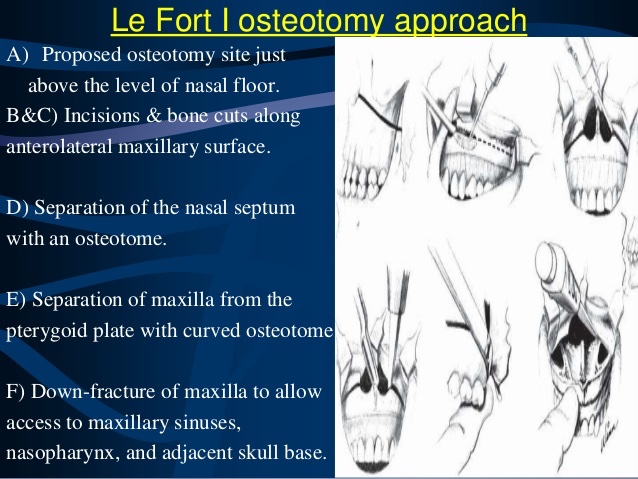
👉Lefort I osteotomy:
- In this approach through a sublabial incision:
- A transverse maxillary osteotomy is performed through both maxillary sinuses:
- Allowing the whole hard palate and both inferior maxillae to be down fractured
- A transverse maxillary osteotomy is performed through both maxillary sinuses:
- Access to the central skull base and nasopharynx is ensured without any visible facial scars
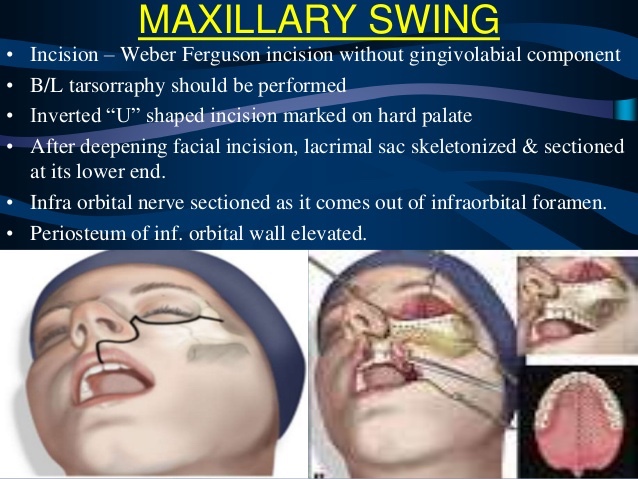
👉Maxillary swing approach:
- This is one of the common approaches to the nasopharynx
- It exposes the nasopharynx and surrounding areas:
- From the anterolateral aspect
- Through a Weber Ferguson incision:
- The maxilla is separated from its bony attachments and swung laterally intact with the masseter muscle and cheek flap
- Access to the opposite side can be established by removing the posterior portion of nasal septum
- After tumor resection:
- The maxilla is swung back and fixed to facial skeleton
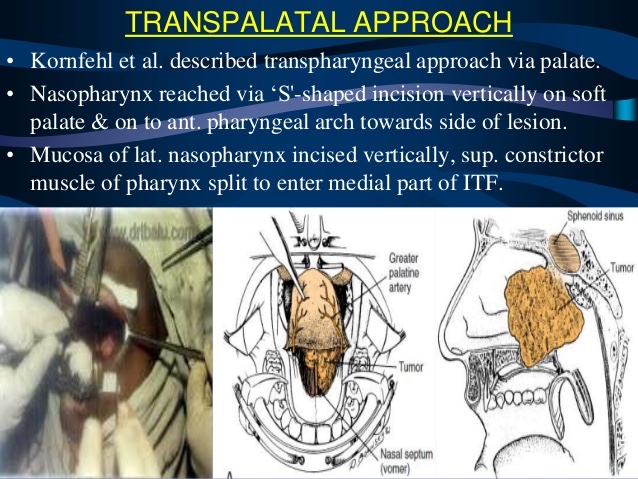
👉Inferior approaches:
- Transpalatal approach:
- The nasopharynx can be accessed by raising a palatal mucoperiosteal flap off the hard palate:
- Separating the soft palate from its bony portion
- The posterior edge of bony hard palate is removed as much as it is necessary:
- To access the nasopharynx
- Greater palatine neurovascular bundle:
- Must be mobilized bilaterally to prevent flap necrosis
- The nasopharynx can be accessed by raising a palatal mucoperiosteal flap off the hard palate:
- Mandibular swing approach:
- This is actually a combination of:
- Transcervical, transmandibular, transpalatal approach:
- Via Frazier incision
- Transcervical, transmandibular, transpalatal approach:
- Soft tissues including parotid gland are elevated from the mandible
- The mid portion of the ascending ramus of the mandible including the coronoid process:
- Is cut and removed to facilitate exposure and to prevent post operative trismus
- The lateral and medial pterygoid muscles are divided to enter the nasopharynx
- Tracheostomy is a must to secure the airway
- Dead space after tumor removal needs to be repaired
- This is actually a combination of:
👉Lateral approach:
- This approach is via the infratemporal fossa:
- This approach is limited by:
- The facial nerve and carotid sheath
- It is used when the tumor extends laterally to involve the parapharyngeal space
- This approach is limited by:
#Arrangoiz #HeadandNeckSurgeon #CancerSurgeon #SurgicalOncologist #HeadandNeckCancer
