
- Basal cell carcinoma (BCC) is the most common type of skin cancer worldwide:
- In the United States, BCC is diagnosed in greater than 2 million patients annually, and global incidence rates continue to rise.
- Risk factors for the development of BCC include:
- Fair skin type
- Exposure to ultraviolet radiation
- Age
- History of BCC
- Genetic disorders:
- Gorlin syndrome
- Xeroderma pigmentosum
- Immunosuppression.
- BCC tumors are generally slow growing and rarely metastasize (less than 0.05%):
- The prognosis for patients who receive appropriate therapy is typically very good.
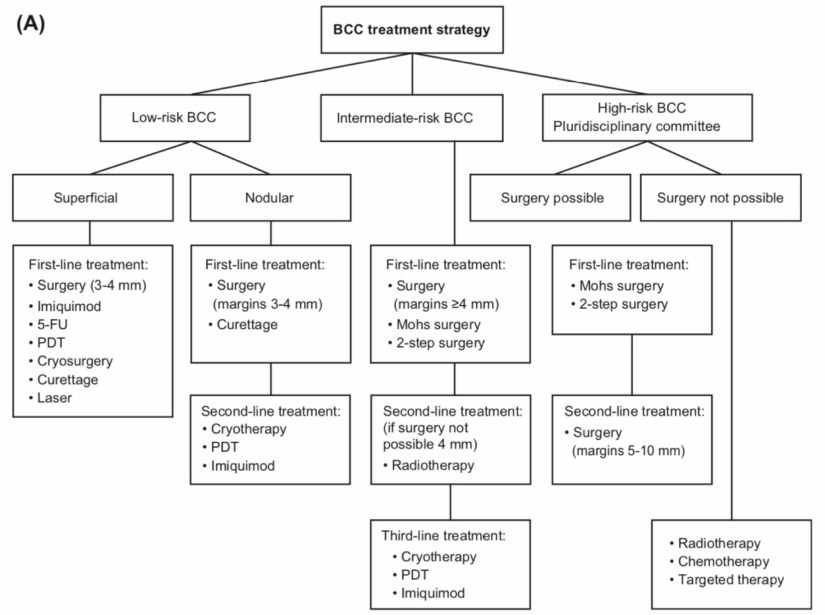
- For most BCCs:
- Including small, well-defined tumors or intermediate-sized, low-risk tumors in low-risk areas:
- The treatment of choice is surgical excision:
- Whereas Mohs micrographic surgery is the preferred surgical technique for:
- Higher-risk tumors
- Recurrent tumors
- Tumors in specific anatomic locations
- Tumors with a wider diameter (Figure).
- Whereas Mohs micrographic surgery is the preferred surgical technique for:
- The treatment of choice is surgical excision:
- Including small, well-defined tumors or intermediate-sized, low-risk tumors in low-risk areas:
- Appropriate use criteria for Mohs micrographic surgery have been developed:
- Mohs is appropriate for patients with:
- Recurrent BCC of any size
- BCC with an unexpected positive margin on recent excision
- Primary aggressive, nodular, or superficial BCC of any size:
- In an area of H (high risk):
- Central face, eyelids, eyebrows, nose, lips, chin, ear, periauricular skin/sulci, temple, genitalia, hands, feet, nail units, ankles, and nipples/areola)
- In an area of M (moderate risk):
- Cheeks, forehead, scalp, neck, jawline, and pretibial surface,:
- With the exception of primary superficial BCC in area M that is 0.5 cm in diameter in otherwise healthy patients:
- For which the appropriateness of Mohs surgery is uncertain;
- With the exception of primary superficial BCC in area M that is 0.5 cm in diameter in otherwise healthy patients:
- Cheeks, forehead, scalp, neck, jawline, and pretibial surface,:
- In an area of L (low risk):
- Trunk and extremities:
- Excluding pretibial surface, hands, feet, nail units, and ankles:
- Mohs is considered appropriate for:
- Aggressive or nodular BCC that is recurrent (of any size)
- BCC that had unexpected positive margins
- Primary aggressive BCC equal or greater than 0.6 cm in diameter
- Primary nodular BCC > 2 cm in diameter in healthy patients or equal or greater than 1.1 cm in diameter in immunocompromised patients.
- Mohs is considered appropriate for:
- Excluding pretibial surface, hands, feet, nail units, and ankles:
- Trunk and extremities:
- Mohs is also considered appropriate for the treatment of primary BCC arising in:
- Previously radiated skin
- Traumatic scars
- Areas of osteomyelitis
- Areas of chronic inflammation / ulceration
- Patients with genetic syndromes
- In an area of H (high risk):
- Mohs is appropriate for patients with:
- Other treatment options include:
- Curettage and electrodessication:
- For small, low-risk, primary BCC
- Superficial field therapies such as:
- 5-fluorouracil
- Imiquimod
- Photodynamic therapy:
- Low-risk, superficial BCC
- Primary or adjuvant radiotherapy:
- Patients for whom surgery is contraindicated or impractical, based on patient considerations,
- For recurrent / perineural disease
- Curettage and electrodessication:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#CancerSurgeon
#CirujanodeCancer
#SkinCancer
#CancerdePiel
#Melanoma
#BasalCellCarcinoma
http://www.sociedadquirurigca.com
