-
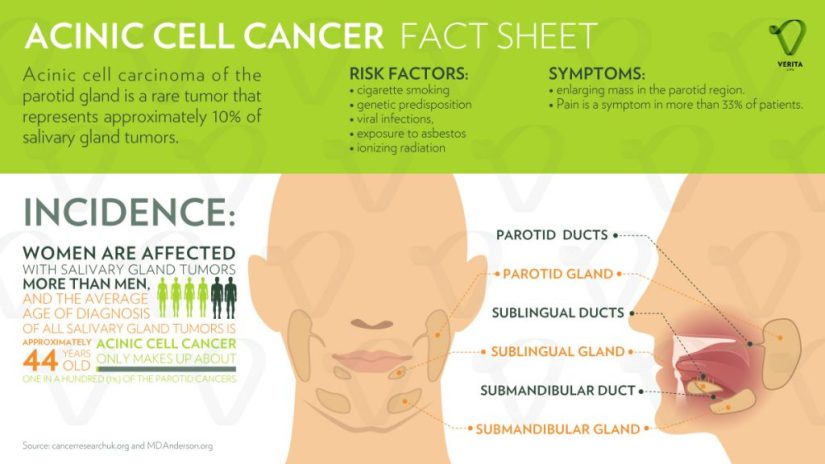
Acinic cell carcinoma (AcCC) is the second most common malignant tumor involving the parotid gland:
-
Representing 15% of malignant parotid gland neoplasms:
-
It accounts for approximately:
-
5% to 17% of all salivary gland tumors
-
10% to 17% of all malignant salivary gland tumors
-
-
-
-
The parotid gland is composed almost exclusively of serous type acini:
-
It is the most common site of AcCC:
-
80% to 90% of cases
-
-
Other reported sites are:
-
The palate:
-
Up to 15% of the cases
-
-
Submandibular gland:
-
4% of the cases
-
-
Sublingual gland:
-
1% of the cases
-
-
-
-
AcCC occurs most often in:
-
The fifth decade of life
-
In women more often than in men (ratio 3:2)
-
-
It is generally a low-grade carcinoma with indolent behavior.
-
Recurrences are usually delayed, sometimes after decades:
-
In a series reported by Ellis et al:
-
12% of tumors recurred
-
8% metastasized:
-
Regional lymph nodes, bone, lung, and brain:
-
The regional lymph nodes were the most common site of metastases:
-
Spafford et al. reported cervical lymphadenopathy to be present in 10% to 15% of cases of AcCC and Spiro et al. in a series of 67 cases with AcCC treated before 1968, identified five cases (7.5%) with cervical metastases at the time of initial treatment.
-
-
-
-
-
-
It is interesting that this tumor is the most common bilateral malignant salivary gland neoplasm:
-
Although its bilateral presentation is not nearly as common as the bilateral presentations of benign tumors:
-
Warthin’s tumor and pleomorphic adenoma
-
-
-
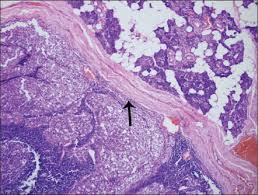
AcCC are typically encased in a fibrous capsule:
-
Grossly resembling round circumscribed nodules with a tan surface:
-
The cut surface is solid but may show cystic degeneration and hemorrhage
-
-

-
Histologically, there are five cell types:
-
Serous acinar cells (explaining the predilection for the parotid gland)
-
Cells with clear cytoplasm
-
Intercalated ductal cell
-
Nonspecific glandular cell
-
Vacuolated cell
-


-
The microscopic recognition of AcCC also requires a strong appreciation for its varied growth pattern:
-
There are four histologic growth patterns:
-
Solid
-
Microcystic
-
Papillary
-
Follicular
-
-
Caution must be taken not to misread:
-
The solid pattern as normal parotid parenchyma
-
The papillary-cystic pattern as cystic mucoepidermoid carcinoma
-
The follicular pattern as metastatic thyroid carcinoma
-
-
Serous acinar differentiation is developed most fully in the acinic cell.
-
These cells have dark round nuclei and granular purplish cytoplasm.
-
-
The diagnosis of AcCC may be difficult to establish, especially when some other cell type dominates the histopathology picture:
-
Some examples of this are the predominance of clear cells might cause confusion with mucoepidermoid carcinoma, clear cell adenocarcinoma, and metastatic renal cell carcinoma:
-
In these circumstances, the diagnostic acinic cells can be identified using a periodic acid-Schiff(PAS) reagent (their cytoplasmic secretory granules are PAS positive and diastase resistant).
-
-
-
Overall survival has been crudely estimated to be about 84%:
-
Survival at 5 years has been reported between 76% to 90%, but fell to 56% at 20 years:
-
Emphasizing the need for long-term follow-up
-
-
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British CowdrayMedical Center in Mexico City:
-
Articles and book chapters published by Dr. Arrangoiz on salivary gland neoplasms:
-
Rodrigo Arrangoiz, Pavlos Papavasiliuo, David Sarcu, Thomas J. Galloway, John A. Ridge, Miriam Lango. Current Thinking on Malignant Salivary Gland Neoplasms. Journal of Cancer Treatment and Research. Vol. 1, No. 1, 2013, pp. 8-24. doi: 10.11648/j.jctr.20130101.12
-
Malignant Salivary Gland Neoplasms Literature Review
-
-
He is an expert in the management of salivary gland neoplasms:
-
If you have any questions about salivary gland neoplasms please fill free to ask Dr. Arrangoiz
-




